3349
Simultaneous acquisition of motion-corrected coronary MRA and respiratory-resolved attenuation maps for whole-heart PET-MR imaging1School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 2MR Research Collaborations, Siemens Healthcare, Frimley, United Kingdom
Synopsis
Motion-compensated attenuation correction is fundamental for accurate quantification in cardiac PET imaging. Here we propose a dual-echo water/fat coronary MR angiography acquisition with a motion-corrected reconstruction framework that simultaneously allows visualisation of the coronary anatomy and produces respiratory-resolved high-resolution attenuation maps. Results from healthy subjects show that the motion correction approach improves vessel contrast and sharpness compared to uncorrected water/fat images. Additionally, respiratory-resolved attenuation maps were obtained from motion fields and water/fat images with good tissue contrast. The proposed scheme can potentially be used for accurate and highly efficient whole-heart motion-corrected cardiac PET-MR imaging ensuring alignment between emission PET, attenuation maps and diagnostic MR data.
Introduction
Simultaneous PET-MR imaging has shown promising results for the assessment of cardiovascular disease by offering complementary anatomical and functional information from both modalities1-3. Clinical PET-MR protocols typically include the acquisition of MR images with various contrasts, while PET is acquired continuously throughout the entire scanning session1. Both PET and MR acquisitions are slower than respiratory motion, so motion compensation techniques are required to minimize blurring and motion artefacts. Moreover, aligned emission and attenuation correction data are required in PET for accurate quantification. In cardiac PET-MR an attenuation map (μ-map), for attenuation correction, is commonly estimated from a segmented water/fat MR image acquired during a ~20s breath hold before the clinical MR protocol. However, changes in the breathing pattern of the subjects during the rest of the examination and/or incomplete breath holds can lead to errors in the μ-map, impacting severely PET image quality. Alternatively, respiratory resolved attenuation maps have been recently proposed3,4. In these approaches, a single or multi-echo MR dataset is acquired throughout the PET acquisition and μ-maps estimated at different respiratory positions are used for motion-resolved attenuation correction. However, the proposed methods did not include preparatory pulses for appropriate tissue contrast and had insufficient spatial resolution, preventing the use of these MR images for diagnostic purposes and leading to long examination times since diagnostic MR images are acquired afterwards. Here we propose a motion-corrected (100% scan efficiency, no data rejection) dual-echo water/fat coronary MR angiography (CMRA), which simultaneously produces respiratory-resolved high-resolution μ-maps and diagnostic quality water and fat coronary MR images.Methods
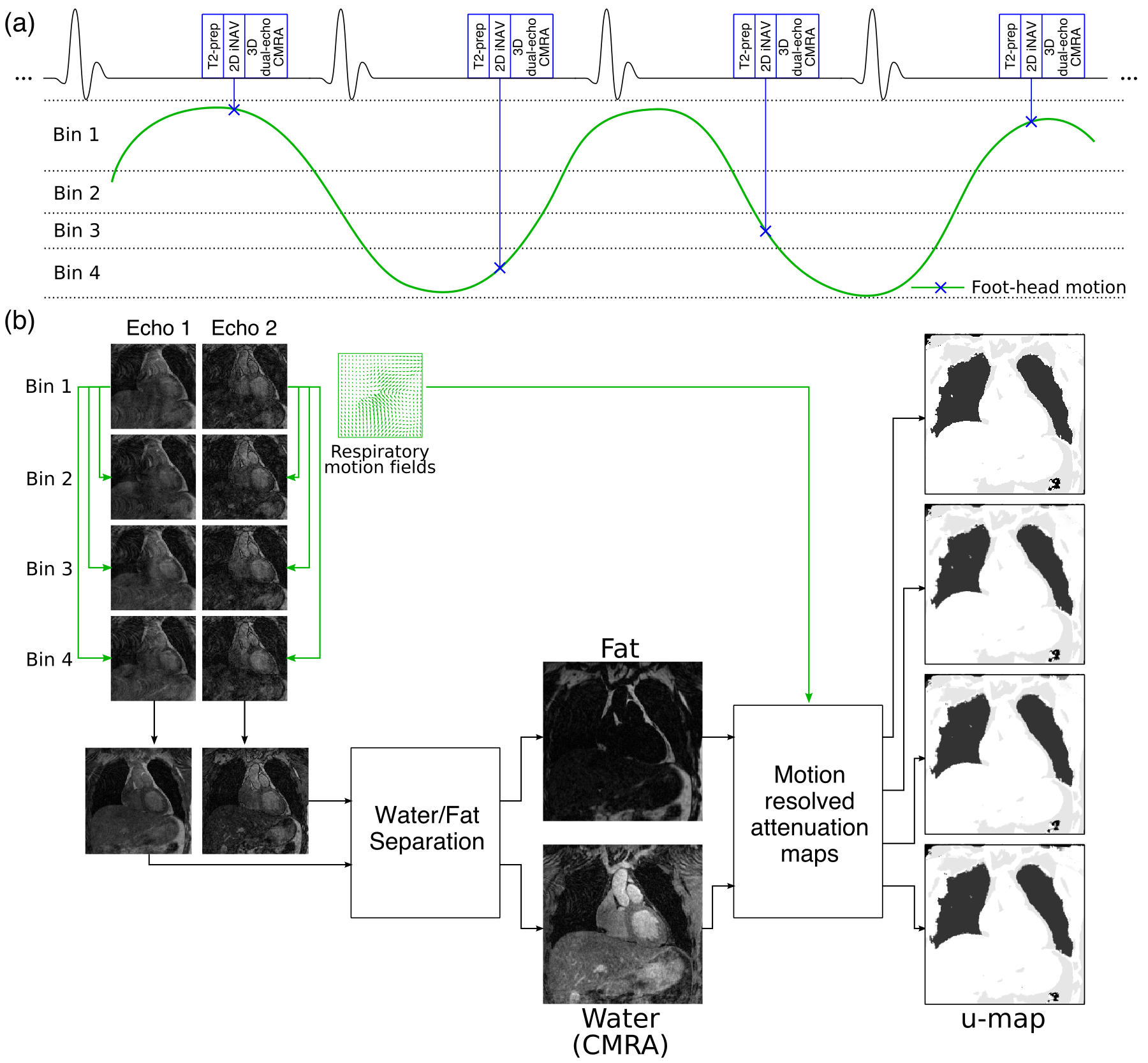
Water/fat coronary MR acquisition consists in an ECG-triggered free-breathing dual-echo 3D T1-weighted spoiled gradient echo sequence (Fig1a). Data is acquired with a fully sampled golden-step Cartesian trajectory with spiral profile order sampling5. In order to improve the contrast between the coronary arteries and surrounding myocardium, an adiabatic T2prep6 pulse is used. 2D image navigators (iNAVs)7 are acquired before the dual-echo acquisition to enable translational beat-to-beat respiratory motion correction in the food-head (FH) and right-left (RL) directions. FH motion is then used to bin the data acquired in each echo in a number of respiratory bins (3-5 depending on the amplitude of the FH motion) and images are reconstructed for each bin using soft-gated iterative SENSE. Finally, non-rigid motion estimated from the bin images via image registration is incorporated directly in a motion-corrected reconstruction2,8 (Fig1b). Water/fat images are then obtained from the motion-corrected images using a magnitude-based correction for bipolar dual-echo images9. Additionally, respiratory-resolved attenuation-maps are obtained by combining the estimated non-rigid respiratory motion fields and segmented water/fat images10.
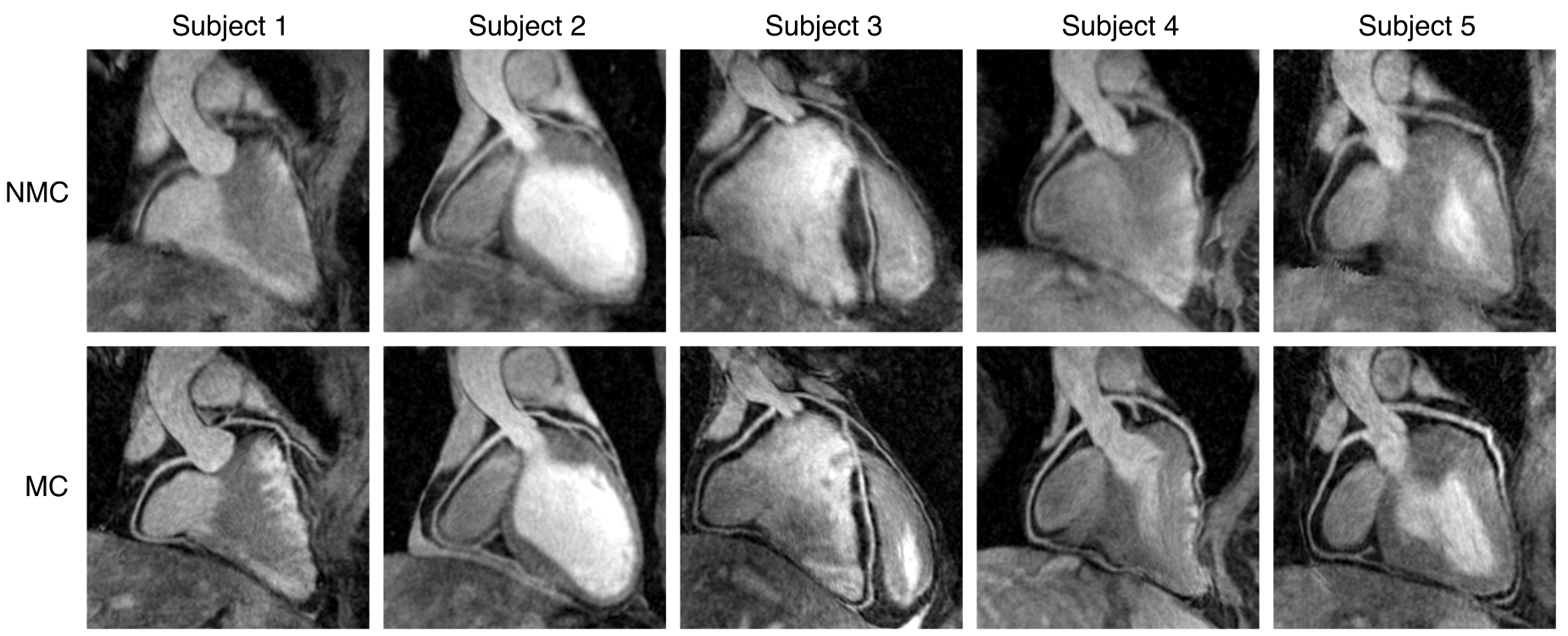
Five healthy subjects were scanned on a Biograph mMR 3T scanner (Siemens Healthcare, Erlangen, Germany) using a prototype implementation of the proposed gradient echo dual-echo CMRA sequence (resolution=1.27mm isotropic, FOV=306x306x90-102mm, coronal orientation, TR/TE1/TE2= 5.26/2.46/3.69ms, FA=20°, T2prep duration=50ms, total acquisition time ~18.3 min). A subject-specific trigger delay and acquisition window (115-153ms) was set coinciding with the mid-diastolic rest period. Images for each echo were reconstructed without motion correction (NMC) and with the non-rigid motion-correction approach (MC). Water/fat images were reformatted to simultaneously visualise the right and left coronary arteries; and the 3D volumes were segmented semi-automatically into three tissue classes (soft-tissue, fat, lungs10) in order to obtain the μ-maps.
Results
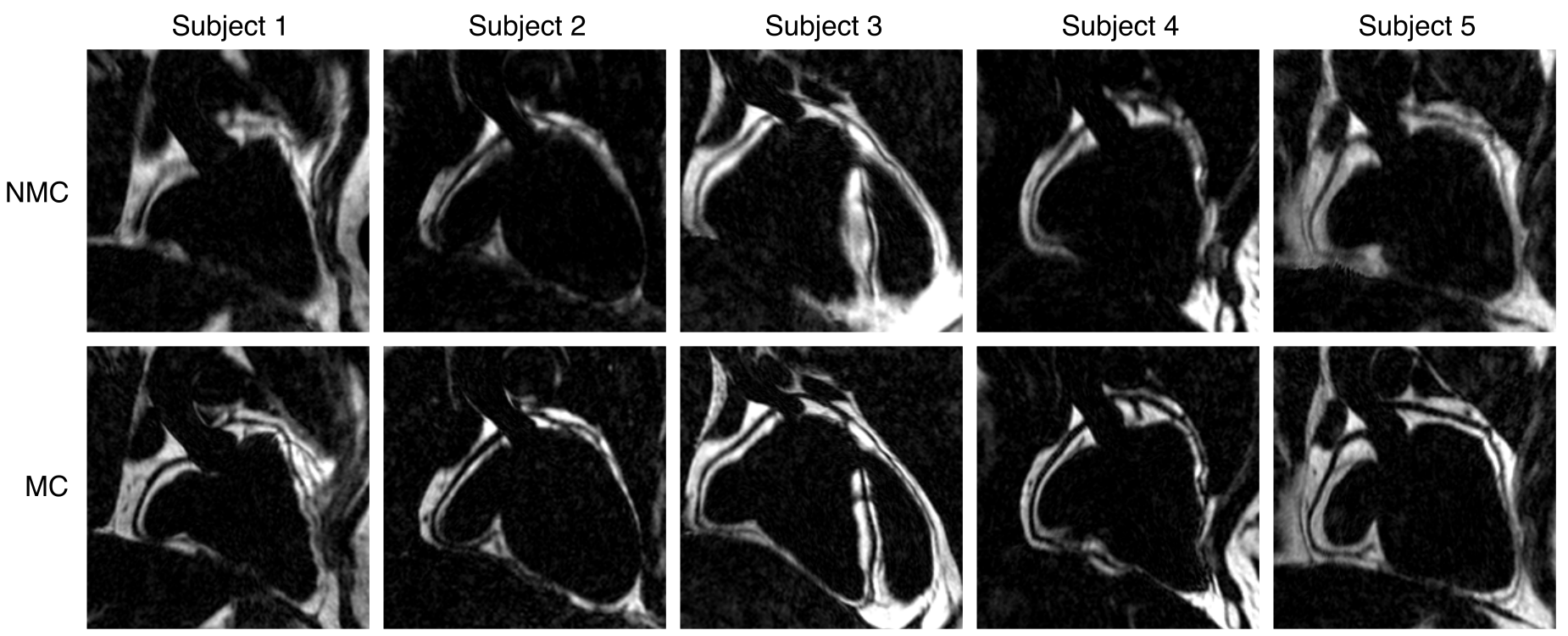
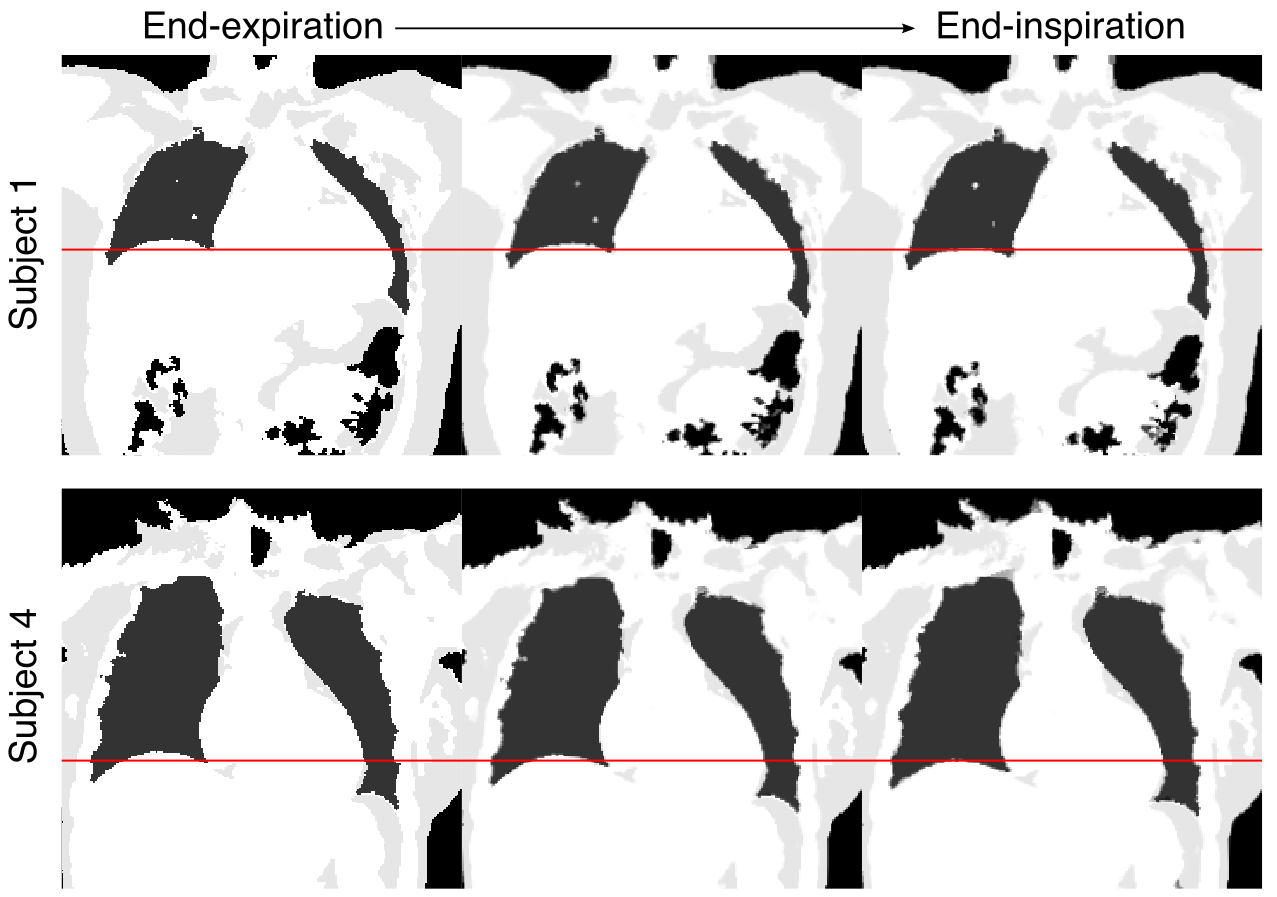
Reformatted water and fat images for all subjects are shown in Fig2 and Fig3 respectively. MC improves image quality, increasing sharpness and visible length of both the right and left coronary arteries in the water images (Fig2) and reducing blurring in the fat images (Fig3), improving contrast between the coronary lumen and surrounding tissue. MC water/fat images offer a good depiction of the thoracic and abdominal anatomy. In particular, epicardial fat, coronary arteries and other relevant cardiac structures are depicted in the water/fat images with high signal to noise ratio and contrast, allowing for the estimation of an accurate high-resolution μ-map (Fig5). By combining the estimated non-rigid respiratory motion fields and the water/fat images, a series of μ-maps at different respiratory positions can be obtained (Fig4), allowing for accurate motion-compensated attenuation correction for cardiac PET-MR imaging.Conclusion
Here we present a free-breathing dual-echo water/fat coronary MR angiography acquisition and reconstruction scheme that allows for visualisation of the coronary anatomy and cardiac fat quantification, that may provide important diagnostic information11, while simultaneously providing motion-resolved attenuation maps for accurate attenuation correction in cardiac PET-MR imaging. The proposed approach provides 100% scan efficiency, as it includes all the acquired data, and has a predictable scan time. Future work will focus on accelerating the acquisition and validating the framework in patients with cardiovascular disease.Acknowledgements
This work is funded by the King’s College London & Imperial College London EPSRC Centre for Doctoral Training in Medical Imaging (EP/L015226/1) and EPSRC Grant EP/N009258/1.References
(1) Rischpler C et al. Hybrid PET/MR imaging of the heart: potential, initial experiences, and future prospects. J Nucl Med 2013;54:402–415
(2) Munoz C et al. Motion-corrected simultaneous cardiac positron emission tomography and coronary MR angiography with high acquisition efficiency. Magn Reson Med 2017. doi:10.1002/mrm.26690
(3) Robson PM et al. Coronary Artery PET/MR Imaging. Feasibility, Limitations, and Solutions. JACC Cardiovasc Imaging 2016. doi:10.1016/j.jcmg.2016.09.029
(4) Kolbitsch C et al. Fully integrated 3D high-resolution multicontrast abdominal PET-MR with high scan efficiency. Magn Reson Med 2017. doi:10.1002/mrm.26757
(5) Prieto C et al. Highly efficient respiratory motion compensated free-breathing coronary MRA using golden-step Cartesian acquisition. J Magn Reson Imaging 2015;41:738–746
(6) Botnar RM et al. Improved coronary artery definition with T2-weighted, free-breathing, three-dimensional coronary MRA. Circulation 1999;99:3139–3148
(7) Henningsson M et al. Whole-heart coronary MR angiography with 2D self-navigated image reconstruction. Magn Reson Med 2012;67:437–445
(8) Cruz G et al. Highly efficient nonrigid motion-corrected 3D whole-heart coronary vessel wall imaging. Magn Reson Med 2016. doi:10.1002/mrm.26274
(9) Liu J et al. Method of B0 mapping with magnitude-based correction for bipolar two-point Dixon cardiac MRI. Magn Reson Med 2017;78:1862–1869
(10) Martinez-Möller A et al. Tissue classification as a potential approach for attenuation correction in whole-body PET/MRI: evaluation with PET/CT data. J Nucl Med 2009;50:520–6
(11) Kellman P et al. Multiecho Dixon fat and water separation method for detecting fibrofatty infiltration in the myocardium. Magn Reson Med 2009;61:215–221
Figures