3338
Subtle differences in left ventricular cardiotoxicity remodeling between risk groups of cancer survivors based on strain analysis from cine-DENSE MRI1Mechanical Engineering, Polytechnique Montreal, Montreal, QC, Canada, 2Biomedical Engineering, University of Virginia, Charlottesville, VA, United States, 3Research Center, Montreal Heart Institute, Montreal, QC, Canada, 4Kinesiology, University of Montreal, Montreal, QC, Canada
Synopsis
The aim of this study was to evaluate a reliable clinical tool to assess subtle differences in left ventricular cardiotoxicity remodeling in acute lymphoblastic leukemia survivors. Cine-DENSE MRI provided accurate evaluation of heart’s functionality of young cancer survivors in the short-axis view. Significant strain differences between groups were mostly observed in basal septal and apical septal segments while most of the other segments did not show significant differences. The next step of this study will be to include a control group of healthy volunteers.
Introduction
Leukemia is the most common form of childhood cancer and acute lymphoblastic leukemia (cALL) has the highest incidence rate. Chemotherapy treatments of cALL include doxorubicine, a drug known to cause long term cardiotoxicity remodeling of the heart, thus worsening heart functions. The purpose of this study was to evaluate a reliable clinical tool based on strain analysis from cine-DENSE-MRI to assess subtle differences in left ventricular cardiotoxicity remodeling.Methods
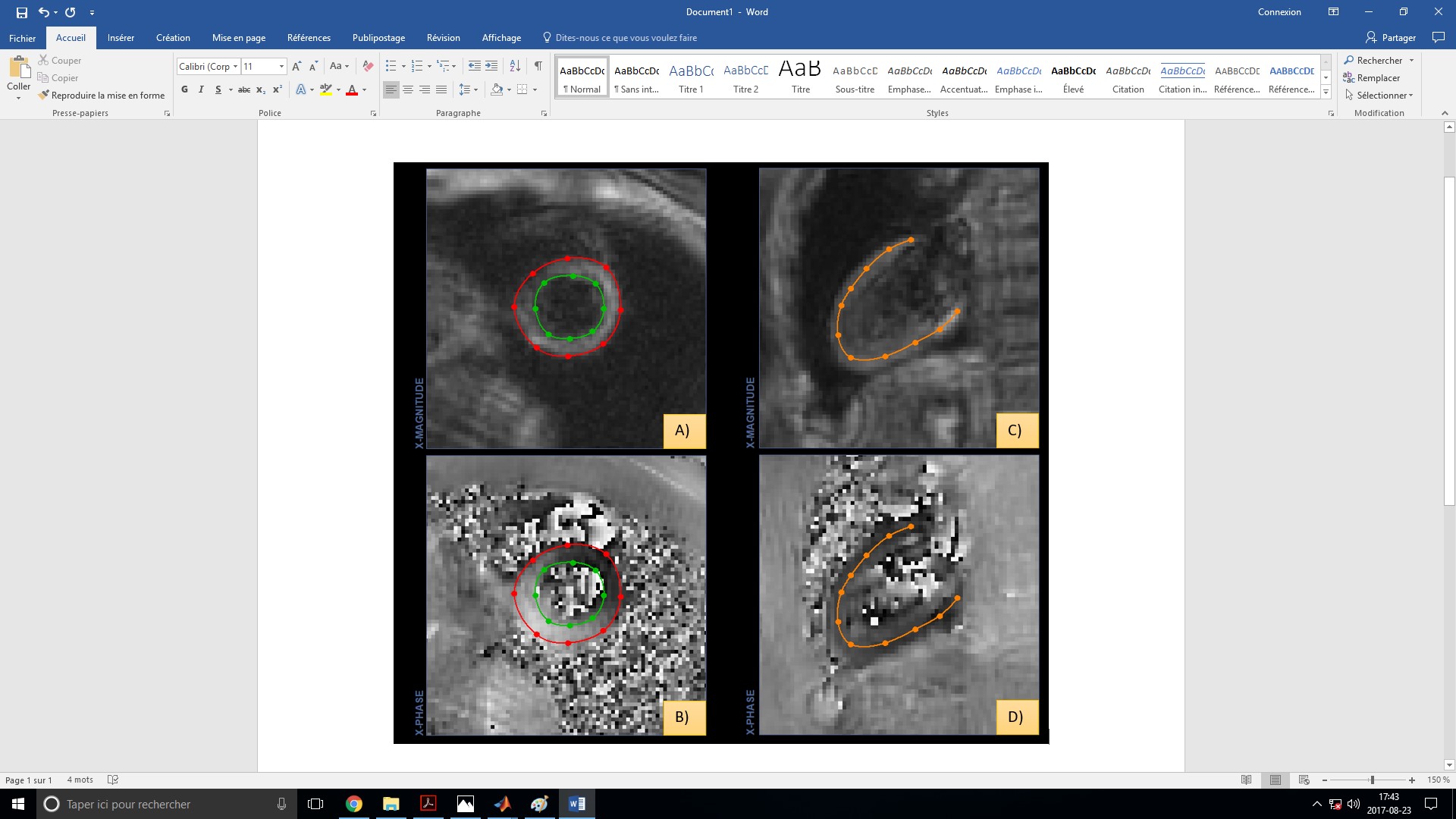
Fourty-six survivors of cALL were prospectively included 13.7±3.7 years after the end of treatment. Data were analyzed according to cALL prognostic risk groups, standard risk (SR, n=10), high risk (HR, n=17) and a high risk group taking into account the administration of dexrazoxane, a cardioprotective agent (HRdex, n=19). All survivors underwent 2D ECG-gated Cine-DENSE-MRI sequences of apical, basal, mid and longitudinal slices of the left ventricle using a clinical 3T MRI system (SkyraTM) and a 18-channel phased array body matrix coil. The sequence parameters included pixel size 2.7x 2.7mm2, slice thickness 8 mm, flip angle 20°, repetition time 15ms, echo time 1ms, temporal resolution 25 frames. Images analysis was performed using the “DENSE-analysis” software [1]. Myocardial contours were semi-automatically segmented based on the 17 segments ventricular model in short-axis and a 4 segments model in long-axis (Figure 1). Data sets were kept and analyzed based on the quality of the cine-DENSE images obtained while data unfit for analyze was discredited. Studied parameters included middle and average tissue radial strain (Err), circumferential strain (Ecc), principal strain (E1), secondary strain (E2) and ventricular torsion throughout the cardiac cycle. Furthermore, end systolic frame was determined by lowest ventricular volume and end systolic strain were evaluated. A repeatability study was conducted to rule out any effects on results caused by the operator’s segmentation amongst subjects. The comparison between groups was performed using a repeated measures analysis of variances for strain data throughout the cardiac cycle and a one way analysis of variances for end systolic strain.Results
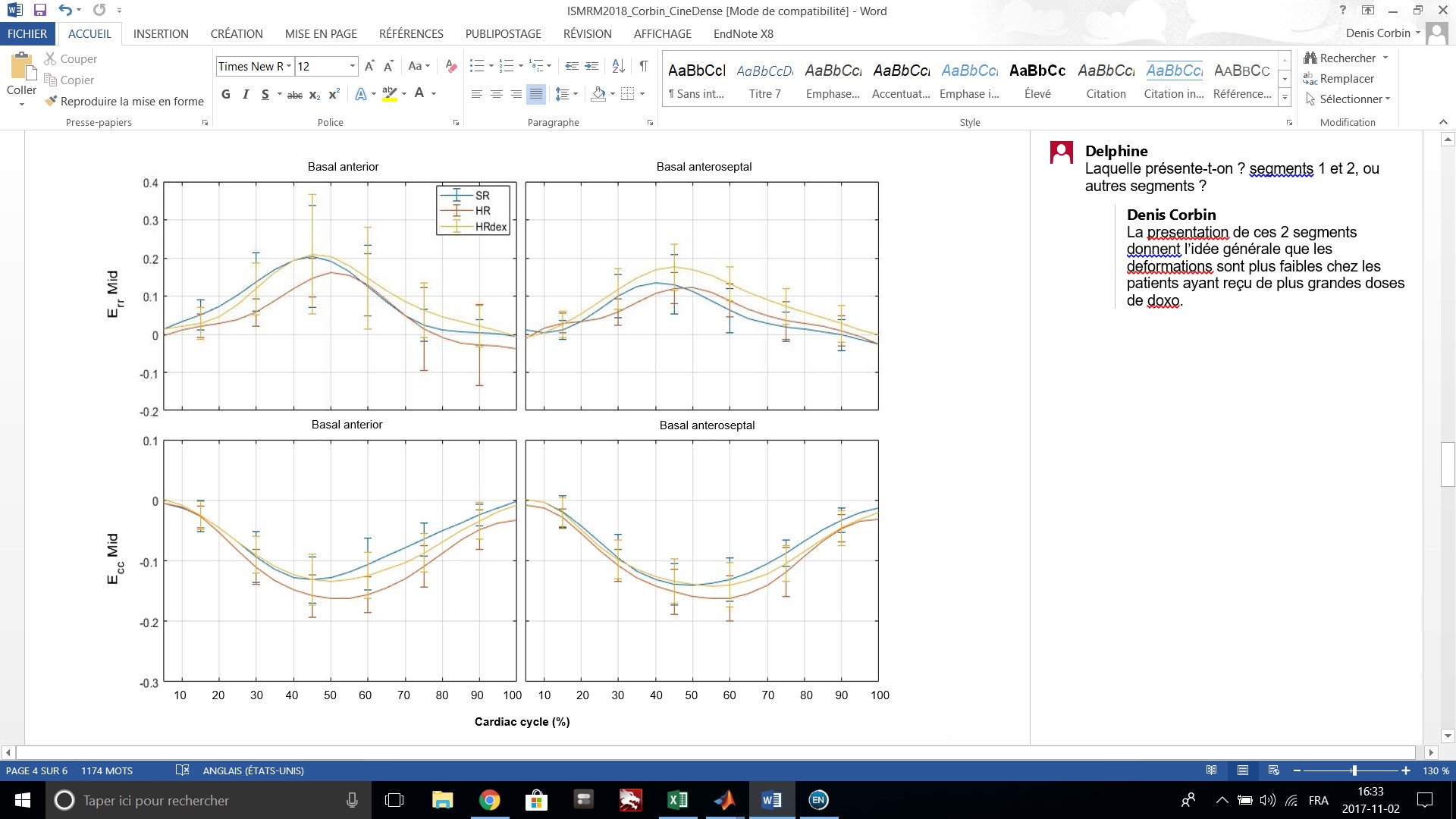
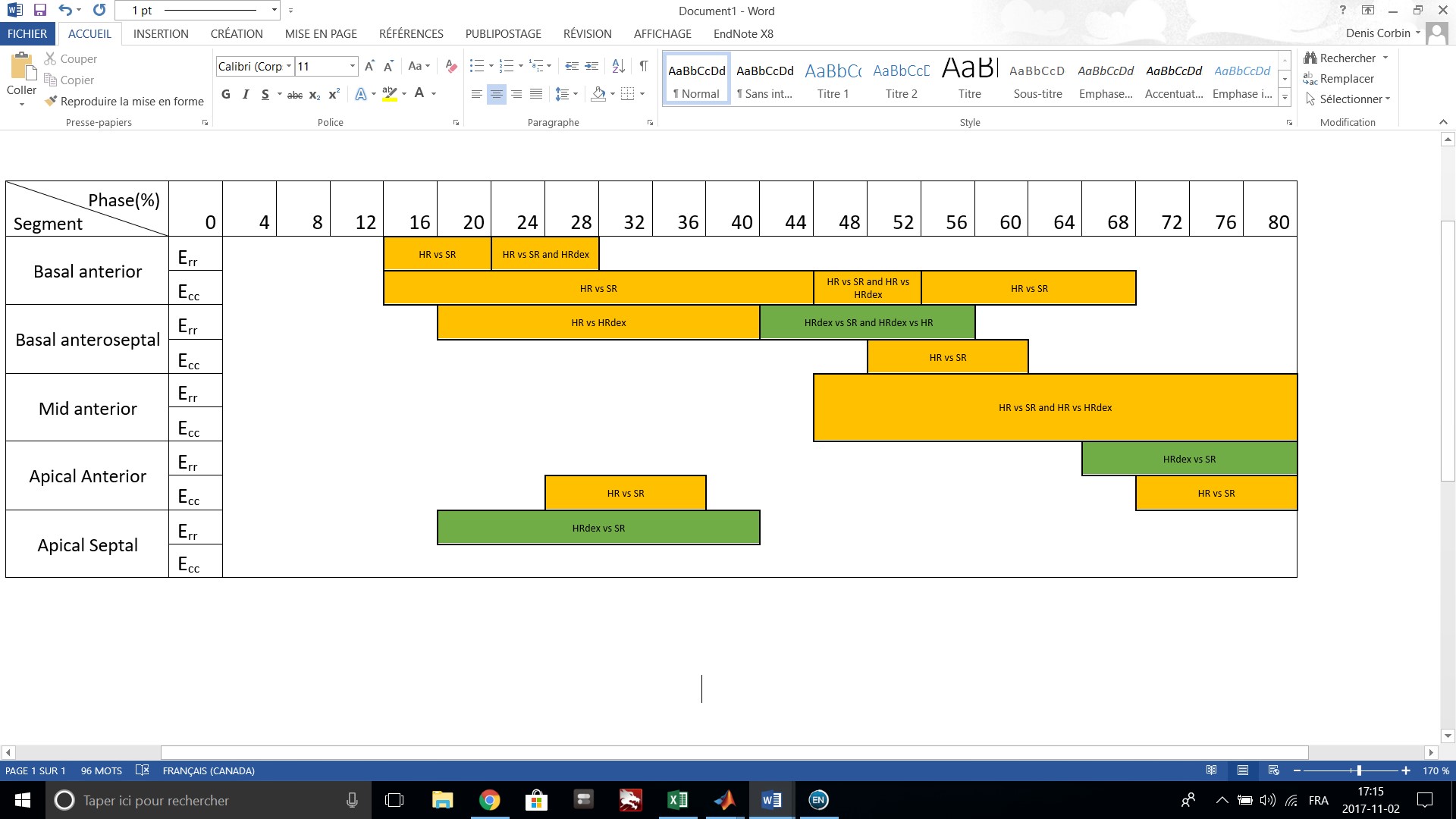
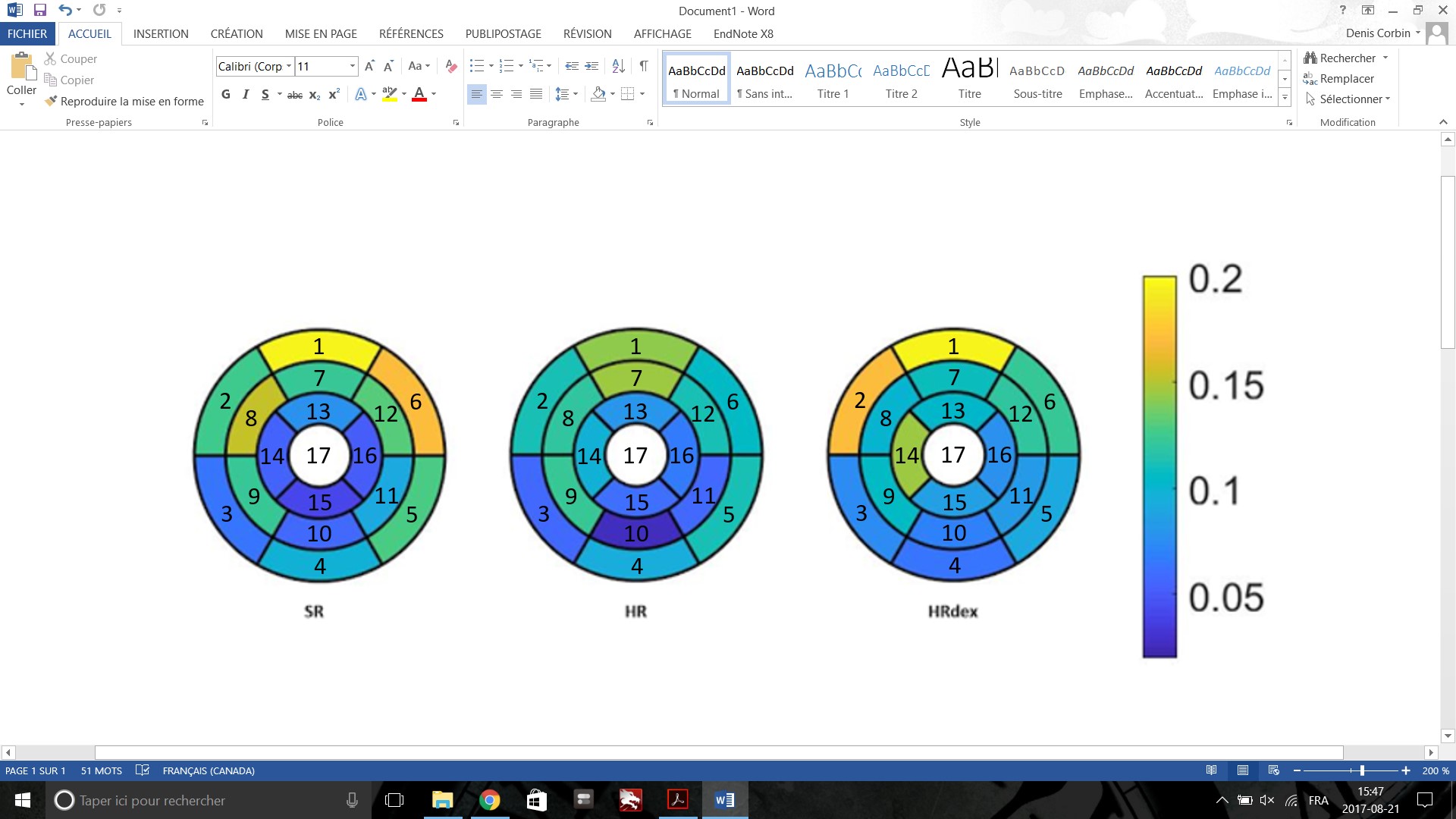
Intra-class coefficients (ICC) showed good to excellent reproducibility (0.753-0.998) across the 17 segments model. Strain patterns along the cardiac cycle were found similar (Figure 2). However, parts of the cardiac cycle showed significant differences between the groups (p<0.05, Figure 3), mainly for the middle and average radial strain in the basal anterior, basal anteroseptal, apical anterior and apical septal segment. Smaller strain were found in the HR group and higher strain were found in the HRdex group as compared to the SR group. End systolic radial and principal strain (Figure 4) were higher for the HRdex group as compared to the HR group for the basal anteroseptal segment and also higher for the HRdex group as compared to the SR group for the apical septal segment (p<0.05). No significant differences were observed for other segments nor other parameters in the short-axis view and in the long axis-view.Discussion
Cine-DENSE MRI provided accurate evaluation of heart’s functionality of young cancer survivors in the short-axis view. Significant strain differences between groups were mostly observed in basal septal and apical septal segment while most of the other segments did not show significant differences. This may be due to cardiac morphologic and functional changes to septum wall induced by cumulative anthracycline dose, thus preventing wall thickening and increasing relative stress [2, 3]. Global myocardial systolic strain values averaged 10% which is in accordance with other studies [4]. Observed differences in the peak basal and apical septal strain can be explained as above. As expected and accepted in other studies, radial strain globally showed that higher strains value were associated with lower anthracycline cumulative dose [5] while the opposite was observed for circumferential strains which may be also caused by morphological changes in the myocardial matrix. Sequence parameters were not optimal, thus forcing us to give up on 20% of our data toward the end of the cardiac cycle for every patient due to a poor signal to noise ratio. Furthermore, an average of 30% of the available data sets in each group were removed from the study due to obnoxious artefact’s presence in images.Conclusion
Our study highlighted that cine-DENSE MRI can effectively show some subtle left ventricular cardiotoxicity remodeling in cancer survivors. The next step of this study will be to include a control group of healthy volunteers in order to truly assess the clinical viability of the strain approach.Acknowledgements
NSERC for the financial support, researchers from the PETALE study for the opportunity to do this complementary MRI sequence on the cancer survivors.References
1. Spottiswoode, B.S., et al., Tracking myocardial motion from cine DENSE images using spatiotemporal phase unwrapping and temporal fitting. IEEE Trans Med Imaging, 2007. 26(1): p. 15-30. 2. McGowan, J.V., et al., Anthracycline Chemotherapy and Cardiotoxicity. Cardiovasc Drugs Ther, 2017. 31(1): p. 63-75.
3. Chatterjee, K., et al., Doxorubicin cardiomyopathy. Cardiology, 2010. 115(2): p. 155-62.
4. Collier, P., D. Phelan, and A. Klein, A Test in Context: Myocardial Strain Measured by Speckle-Tracking Echocardiography. Journal of the American College of Cardiology, 2017. 69(8): p. 1043-1056. 5. Scully, R.E. and S.E. Lipshultz, Anthracycline cardiotoxicity in long-term survivors of childhood cancer. Cardiovascular Toxicology, 2007. 7(2): p. 122-128.
Figures