3332
Importance of Right Atrial Strain on Right Ventricular Dilation in Pediatric and Adult Patients with Repaired Tetralogy of Fallot: Fast CMR Feature Tracking StudyShuang Leng1, Liwei Hu2, Xiaodan Zhao1, Ju Le Tan1,3, Wen Ruan1, Ru San Tan1,3, Yumin Zhong2, and Liang Zhong1,3
1National Heart Centre Singapore, Singapore, Singapore, 2Shanghai Children Medical Centre, Shanghai Jiaotong University, Shanghai, China, 3Duke-NUS Medical School Singapore, Singapore, Singapore
Synopsis
Right ventricular (RV) volume overload is common in patients after initial repair of tetralogy of Fallot (rTOF) and is associated with adverse long-term outcomes. We aimed to determine the effect of right atrial (RA) strain derived from feature tracking cardiovascular magnetic resonance (CMR) on the RV volume in both pediatric and adult rTOF patients. Results revealed that RA strain and strain rates were impaired in rTOF and RA reservoir strain impairment was significantly associated with RV dilatation. Hence, unloading of the RA and augmentation of RA function may be important future therapeutic targets in rTOF.
Introduction
Right ventricular (RV) volume overload from residual pulmonary regurgitation in patients after repair of tetralogy of Fallot (rTOF) portends adverse outcomes. Longitudinal cardiovascular magnetic resonance (CMR) monitoring of RV volumes is obligatory for timing of pulmonary homograft replacement. Recent reports of CMR feature-tracking for left atrial function assessment pave the way for its application in the right atrium (RA). We aimed to study the relationship between CMR-assessed RV volumes and RA strain parameters among pediatric rTOF patients compared to healthy control subjects.Methods
Pediatric rTOF patients were prospectively enrolled from a centre in Shanghai; and adult rTOF patients and healthy control subjects, from a center in Singapore. All subjects underwent cine CMR using a standardized protocol. Central off-line assessment of ventricular volumes and function was performed using Simpson’s method; and longitudinal RA strain parameters measured using an in-house semi-automatic post-processing algorithm that tracked, on standard four-chamber cine view, the distance (L) between the medial or lateral right atrioventricular junctions and a user-defined point at the mid posterior RA wall (Figure 1). Longitudinal strain (ε) at any time point (t) in the cardiac cycle from end-diastole (time 0) was calculated as: $$$\epsilon(t)=\frac{(L(t)-L_{0})}{L_{0}}\times100\%$$$. RA reservoir strain (εs, atrial reservoir function), passive strain (εe, atrial conduit function) and active strain (εa, atrial contractile booster pump function) were calculated at t equals RV end-systole, RV diastasis and pre-RA systole, respectively, and their corresponding peak strain rates (SR) derived. Student’s t test was used for inter-group comparison; p < 0.05 denotes statistical significance.Results
We enrolled 22 pediatric rTOF (14 males, mean age 8.9 ± 3.8 years), 57 adult rTOF (20 males, mean age 37.3 ± 13.7 years), and 53 control subjects (11 males, mean age 39.4 ± 16.6 years). Pediatric rTOF patients had similar left ventricular (LV) end-diastolic volume index (EDVi), LV end-systolic volume index (ESVi), and LV ejection fraction (EF) in comparison to adult rTOF patients and normal controls. The group of adult rTOF had significantly reduced LVESVi and LVEF compared to normal subjects. For RV function, both pediatric and adult rTOF patients had significantly larger RVEDVi and RVESVi in comparison to normal controls, but only the adult rTOF had significantly lower RVEF than controls. Seventy-two percent (41/57) of adult rTOF patients had pulmonary regurgitation (PR) fraction larger than 30%, while in pediatric patients, 82% (18/22) had PR fraction larger than 30%. RA strain analysis processing time averaged 1.5 minutes per subject. Intra- and inter-observer variations were between 2.1% to 4.9% (all ICC > 0.90). RA strains and strain rates were similar between pediatric and adult rTOF patients; but in both groups, were significantly reduced compared to controls (Table 1). RA strains and strain rates were inversely correlated with RVEDVi (all p < 0.05). On multivariate analysis, RA reservoir strain (β = -2.03 for εs, p < 0.0001) and age (β = -0.375 for Age, p = 0.038) remained independent predictors of RVEDVi after adjusting for other parameters. Given the same age and with one percent decrease in RA reservoir strain, the RVEDVi was found to increase by 2.03 ml/m2.Discussion
The atria play a significant role in cardiac performance. Present study shows the feasibility of RA strain measurement in rTOF by CMR feature tracking. Abnormal RA function in both pediatric and adult rTOF was revealed by lower RA strain and strain rates in all phases compared to normal controls. The negative correlation of RA reservoir strain with RVEDVi has shown that reduced atrial function is significantly related with volume-loaded ventricles.Conclusion
In rTOF, RA strain parameters are impaired, and RA reservoir strain impairment is associated with RV dilatation. These strain parameters, which are highly reproducible and can be derived rapidly from post-processing of standard four-chamber cine CMR images, are promising candidate indices for noninvasive detection of RA dysfunction, monitoring of disease progression and response to treatment in rTOF patients.Acknowledgements
No acknowledgement found.References
No reference found.Figures
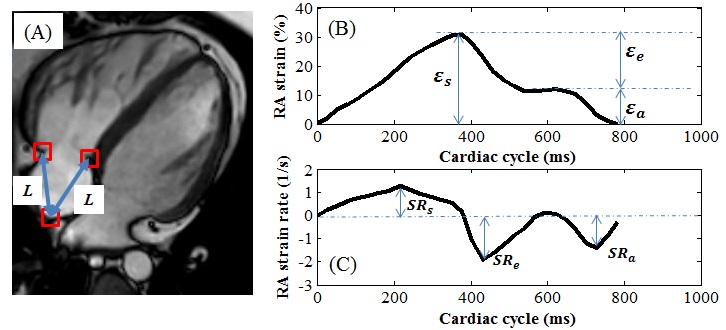
Figure 1. (A) Four-chamber
cine image showing feature tracking of the distance (L) between right ventricular septum or free wall and the right
atrial wall (red boxes). Graphs depict time-varying longitudinal strain (B) and
its first derivative (C), from which strain parameters (ε) and their corresponding peak strain rates (SR) at various cardiac
phases (see text) can be read off.
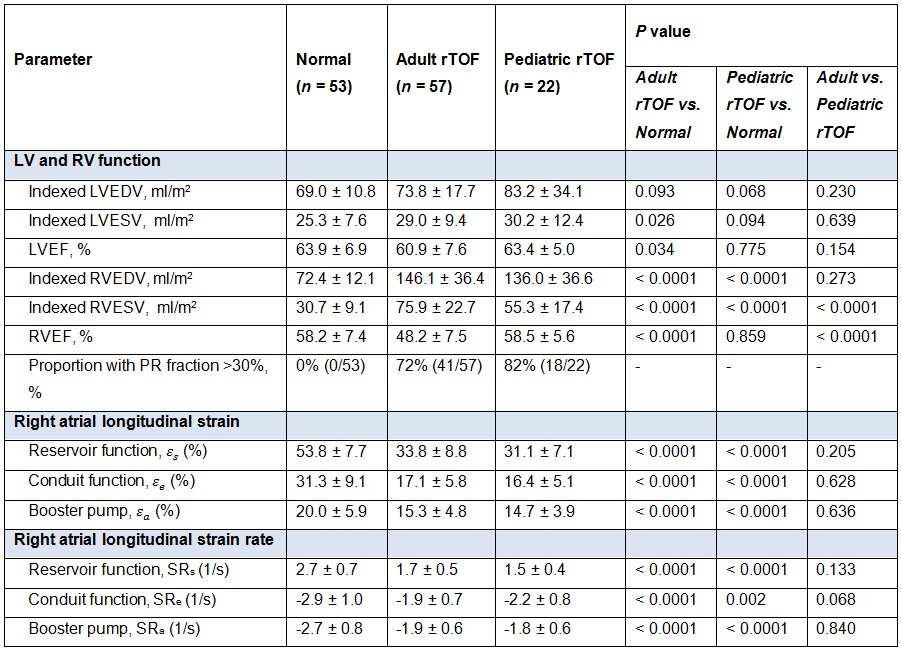
Table 1. Comparison of ventricular and right atrial strain parameters among
groups. Data are presented as mean ± SD. LV: left
ventricular; RV: right ventricular; EDV: end-diastolic volume; ESV:
end-systolic volume; EF: ejection fraction; PR: pulmonary regurgitation; ε: longitudinal
strain; SR: longitudinal strain rate; rTOF: repaired tetralogy of Fallot.