3326
Radial-CAIPI myocardial first-pass perfusion for high spatiotemporal resolution “iso-phase” multi-slice imaging at multiple cardiac phases per cycle1NHLI, Imperial College London, London, United Kingdom, 2CRC, Royal Brompton Hospital, London, United Kingdom, 3BHF Glasgow CRC, University of Glasgow, Glasgow, United Kingdom
Synopsis
A high-resolution myocardial perfusion sequence is implemented with radial-CAIPI to allow simultaneous acquisition of the conventional three myocardial slices, all at identical cardiac phase, which can be repeated for multiple phases of the cardiac cycle and throughout the first-pass. The synchronised cardiac phases and repeat acquisitions aim to enable improved specificity, through better artifact identification.
Introduction
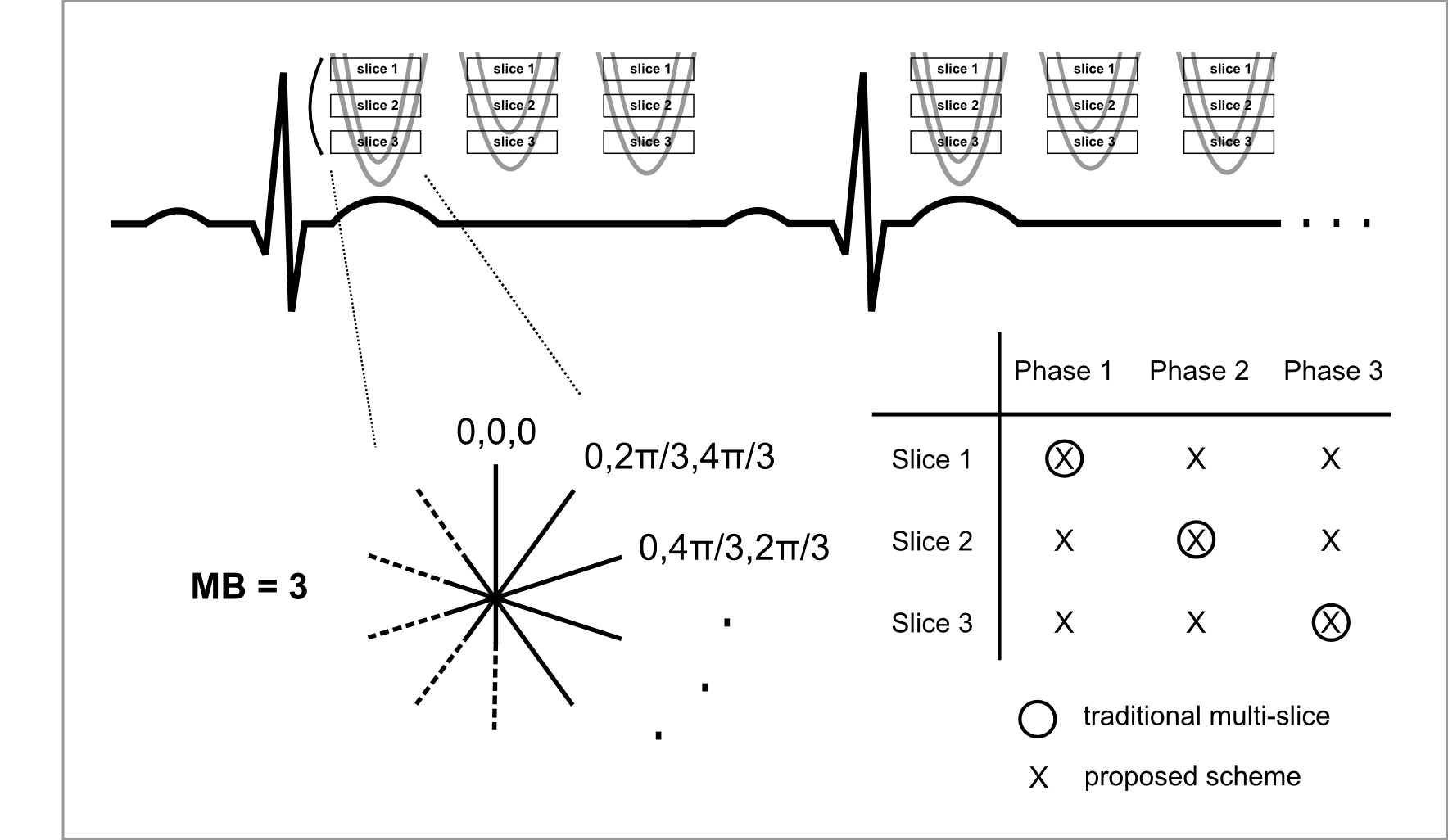
Clinical multi-slice first-pass myocardial perfusion typically acquires three or four slices every cardiac cycle, each slice at a different phase of the cycle.
The variation in cardiac phase between the slices significantly complicates clinical reading by introducing confounding factors: different motion artifacts, changing myocardial thickness, and long-axis cardiac motion of myocardial tissue1.
Simultaneous multi-slice (SMS) techniques2, including CAIPIRINHA (“CAIPI”) extensions3, accelerate 2D sequences by acquiring multiple slices simultaneously. These techniques have previously been applied in myocardial perfusion to increase myocardial spatial coverage during each cycle4,5 by simultaneously collecting a different 2 or 3 slices at each acquired cardiac phase. These approaches acquire more slice locations each cycle, but at a mixture of cardiac phases.
Consistent cardiac phase is one hypothesised advantage of 3D myocardial perfusion imaging6, but 3D demands increased shot duration. Applying the consistent cardiac phase advantage to 2D could significantly benefit diagnostic accuracy.
SMS techniques allow acquisition of multiple slices with identical cardiac timing (“iso-phase”).The proposed method is aimed at improving specificity by repeatedly acquiring the same SMS slices at multiple phases of the cardiac cycle, using a radial acquisition for its greater compatibility with SMS7 and compressed sensing reconstructions.
Methods
Saturation recovery radial single-shot imaging was optimised for minimal shot duration8. Radial-CAIPI7 was used, applying phase-modulations of 0, 2$$$\pi$$$/3, 4$$$\pi$$$/3 for multi-band (MB) factor 3 (8mm slice thickness, 16mm slice gap). The sequence parameters were: TE/TR: 1.3/2.1ms, Nrays: 48, Shot duration: 101ms, SRT: 100ms, Resolution: ~1.3x1.3mm, FA: 12 degrees. Three cardiac phases were acquired for each set of SMS slices, acquiring 50 first-pass cycles (Figure 1).
A second implementation increased the multiband factor for five slices (thickness=8mm, separation=8mm, [0,2$$$\pi$$$/5,4$$$\pi$$$/5,6$$$\pi$$$/5,8$$$\pi$$$/5] modulation) at each of the three phases. The MB=5 RF pulses were longer to reduce peak voltage, slowing TR to 2.8ms, requiring 36 ray undersampling to maintain shot duration and SAR constraints. The sequence was otherwise consistent with the MB=3 implementation.
For reconstruction (MATLAB, Natick, MA), SMS rawdata was phase demodulated7 to separate the slices. Total-variation temporally constrained compressed sensing9 was used to compensate radial undersampling ($$$\alpha$$$temporal=8x10-3, Niterations=200). The reconstruction gave three (or five) slices, each at three cardiac phases, for all 50 measurements.
Five consenting patients under clinical investigation requiring late-enhancement imaging were recruited for rest perfusion under ethical approval. Four were acquired at MB=3 and one was tested with MB=5. Rest first-pass imaging was performed during antecubital injection of a 1M GBCA (0.1mmol.kg-1) at 3ml.s-1 with 20ml saline flush at 5ml.s-1.
Results
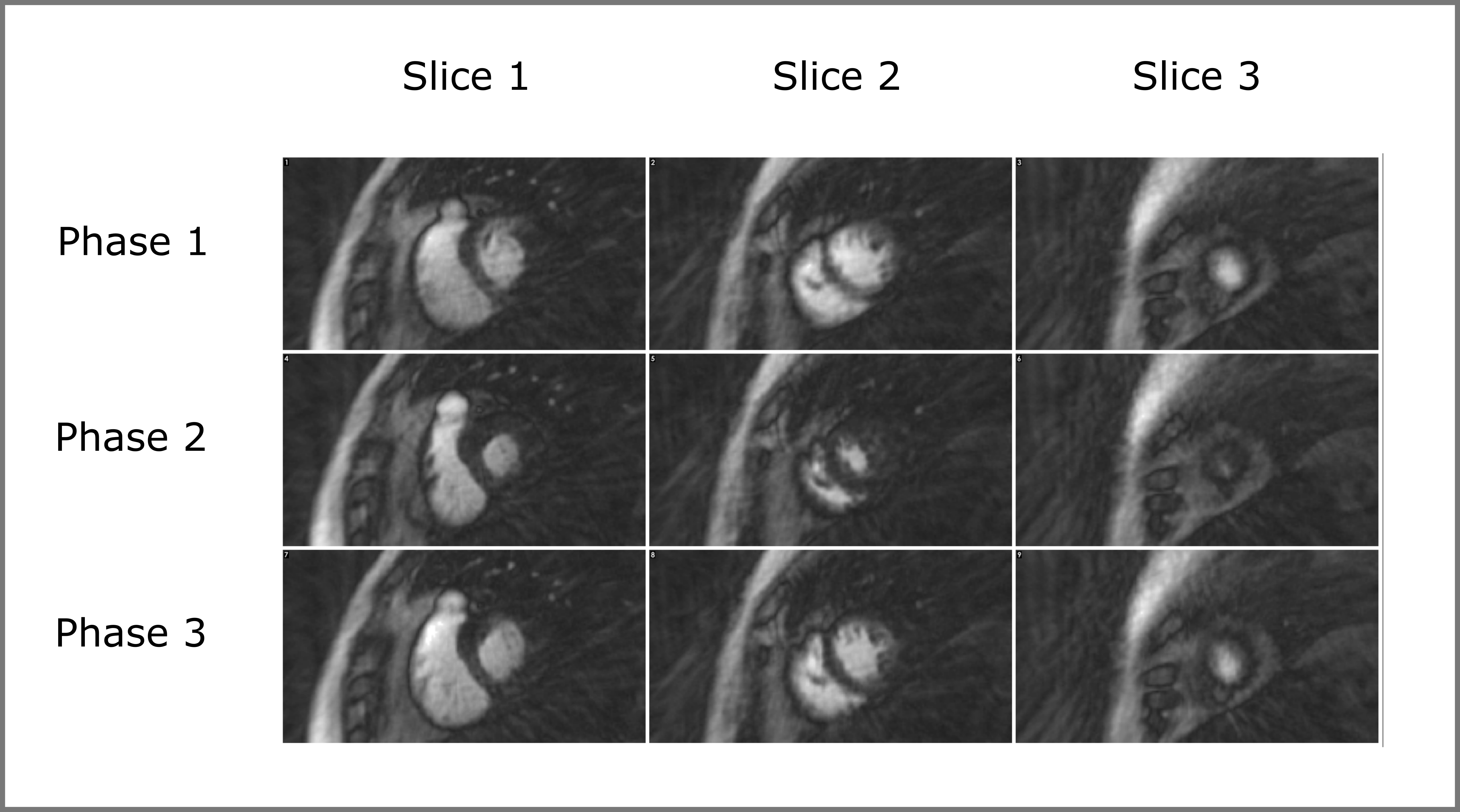
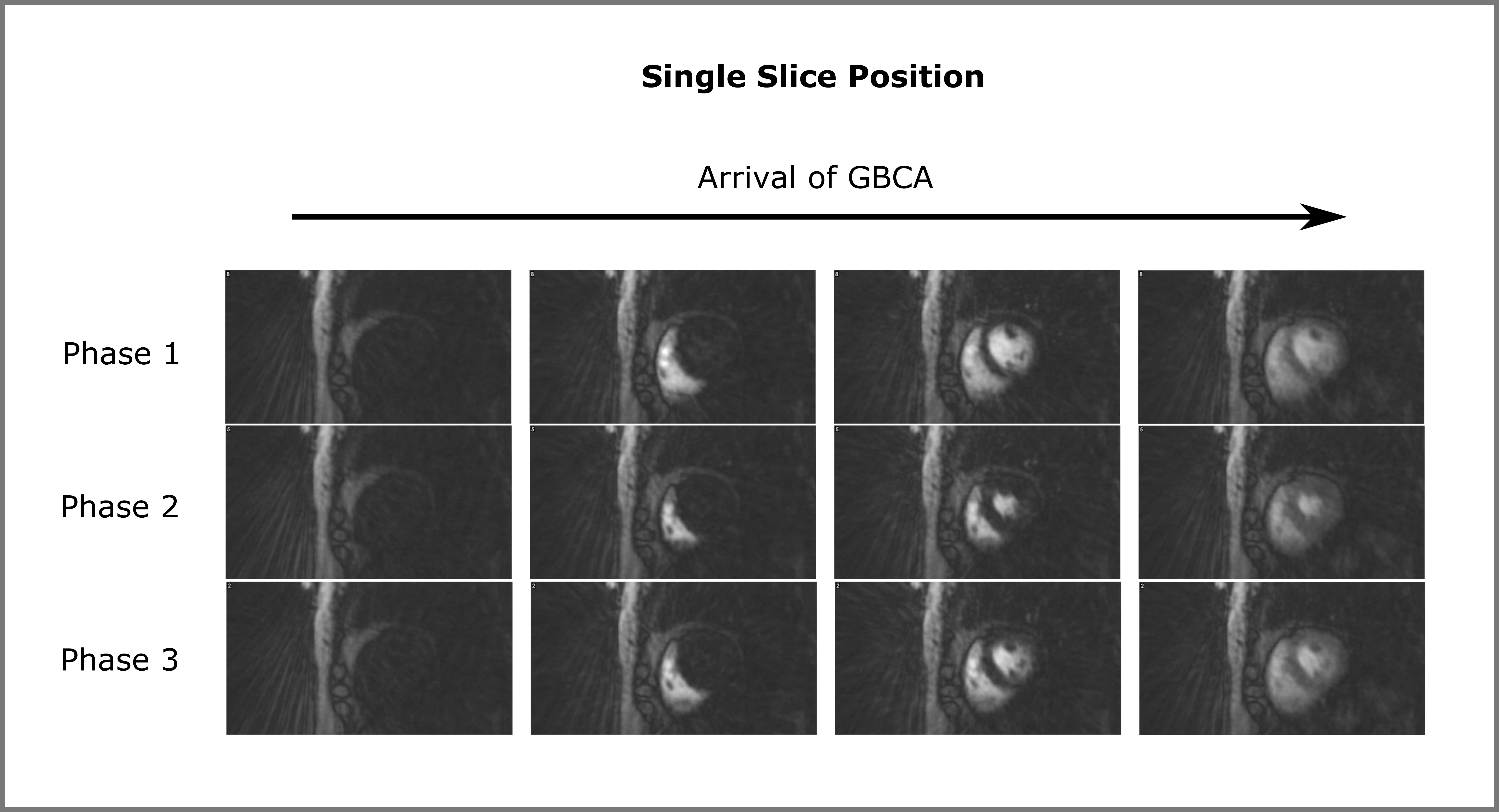
All acquisitions completed successfully. Phase demodulation accurately separated the slices, allowing all three slices to be viewed at the three cardiac phases every cardiac cycle. The compressed sensing reconstruction reduced apparent radial streaking and noise.
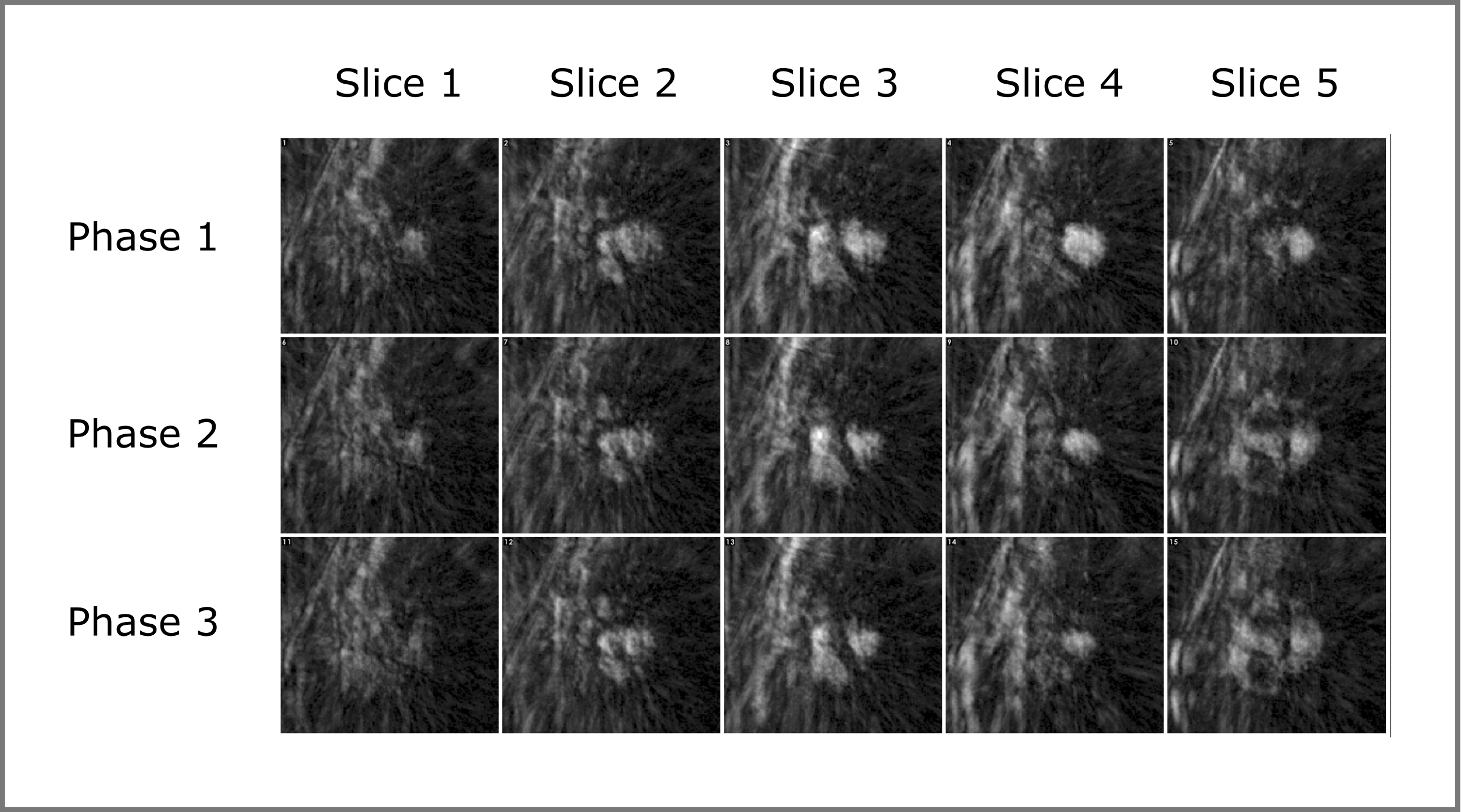
Figure 2 is an example of the 3 slices and 3 phases for a single cardiac cycle. Figures 3 & 4 show multiple cycles for the different phases in a single slice for another patient. Figure 5 shows the five slices and three phases for the MB=5 patient.
Image quality was similar in all MB=3 acquisitions, with occasional artifactual myocardial dark-regions, which differed between cardiac phases. Image quality at MB=5 was markedly reduced, and adjudged non-diagnostic.
Discussion
The accurate separation of slices by radial-CAIPI, even without employing coil sensitivities, is encouraging for this application and supports the feasibility of implementing smaller gaps between excited slices.
The focus of this study was to collect the same slices at multiple cardiac phases, rather than former strategies aiming for more slice locations during the cardiac cycle. The MB=5 sequence aimed to explore extended coverage of the LV myocardium; however, such factors appear too large for cardiac applications5 as further angular undersampling combined with increased MB factor significantly reduced image quality.
There is interest in increased myocardial coverage, as possible in other perfusion techniques, but it is uncertain whether coverage is the optimal approach to improve diagnostic accuracy. Sensitivity of current MR myocardial perfusion techniques is already high10, with suggestions that three (or fewer11) slices are sufficient. Improving specificity through reduction and improved identification of artifacts may be more important. The technique of repeated iso-phase slice-set acquisitions proposed here could potentially be one such method. Investigations in CAD patients at stress are required to test for any improvement in specificity with this technique.
Conclusions
Radial-CAIPI high-resolution acquisition of multiple slices at consistent (“synchronous”) cardiac phase enabled rapid repetition of the same slices at multiple phases of every cardiac cycle. It is proposed that this new approach may assist artifact identification, towards improved specificity in first-pass perfusion.Acknowledgements
The Cardiovascular Research Centre at the Royal Brompton Hospital is supported by Imperial College London.
The Cardiovascular Research Centre at the University of Glasgow is supported by the British Heart Foundation.
References
1. Schwitter J. Myocardial perfusion. J Magn Reson Imag. 2006;24(5):953-963.
2. Larkman DJ, Hajnal JV, Herlihy, AH, et al. Use of multicoil arrays for separation of signal from multiple slices simultaneously excited. J Magn Reson Imag. 2001;13(2): 313-317.
3. Breuer FA, Blaimer M, Heidemann RM, et al. Controlled aliasing in parallel imaging results in higher acceleration (CAIPIRINHA) for multi-slice imaging. Magn Reson Med. 2005;53(3): 684-691.
4. Stäb D, Wech T, Breuer FA, et al. High resolution myocardial first-pass perfusion imaging with extended anatomic coverage. J Magn Reson Imag. 2014;39(6): 1575-1587.
5. Wang H, Adluru G, Chen L, et al. Radial simultaneous multi-slice CAIPI for ungated myocardial perfusion. Magn Reson Imag. 2016;34(9): 1329-1336.
6. Fair MJ, Gatehouse PD, DiBella EVR, et al. A review of 3D first-pass, whole-heart, myocardial perfusion cardiovascular magnetic resonance. J Cardiovasc Magn Reson. 2015;17(1):68.
7. Yutzy SR, Seiberlich N, Duerk JL, et al. Improvements in multislice parallel imaging using radial CAIPIRINHA. Magn Reson Med. 2011;65(6):1630-1637.
8. Roeloffs V, Voit D, Frahm J. Spoiling without additional gradients: Radial FLASH MRI with randomized radiofrequency phases. Magn Reson Med. 2016;75(5): 2094-2099.
9. Adluru G, Awate SP, Tasdizen T, et al. Temporally constrained reconstruction of dynamic cardiac perfusion MRI. Magn Reson Med. 2007;57(6): 1027-1036.
10. Schwitter J, Wacker C, Wilke N, et al. Superior diagnostic performance of perfusion-cardiovascular magnetic resonance versus SPECT to detect coronary artery disease: The secondary endpoints of the multicenter multivendor MR-IMPACT II. J Cardiovasc Magn Reson. 2012;14(1):61.
11. Biglands JD. Quanitifying myocardial blood flow using dynamic contrast enhanced cardiac magnetic resonance imaging. PhD Thesis, University of Leeds. 2012.
Figures