3320
Global left ventricular myocardial deformation measures by CMR tissue tracking in isolated diastolic dysfunction (DD) spontaneous T2DM rhesus monkeys: comparison with tagging1Department of Radiology, Sichuan University, Chengdu, China, 2Sichuan Primed Biotech Group Co., LTD, Chengdu, China, 3Mallinckrodt Institute of Radiology, Washington University School of Medicine, St. Louis, MO, United States
Synopsis
In this study, the myocardial deformation characteristics of early diabetic cardiomyopathy were evaluated by using CMR strain imaging in a spontaneous non-human primate T2DM disease model. We found the early cardiac dysfunction characteristics of diabetic cardiomyopathy, and verified the effectiveness of CMR-tissue tracking in its early diagnosis.
Introduction
Quantitative deformation imaging derived strain can detect myocardial damage beyond that indicated by ejection fraction in the early stage of diabetic cardiomyopathy (DCM).1 CMR tagging is considered the reference standard for the assessment of LV function,2 but limited in clinical applicability for the acquisition of additional tagging sequences and post processing. CMR-tissue tracking (CMR-TT), a new easier operation myocardial strain evaluation method with no additional image acquisition and no increase in scanning time, is possible replace tagging for the evaluation of early cardiac function changes in diabetic cardiomyopathy.Methods
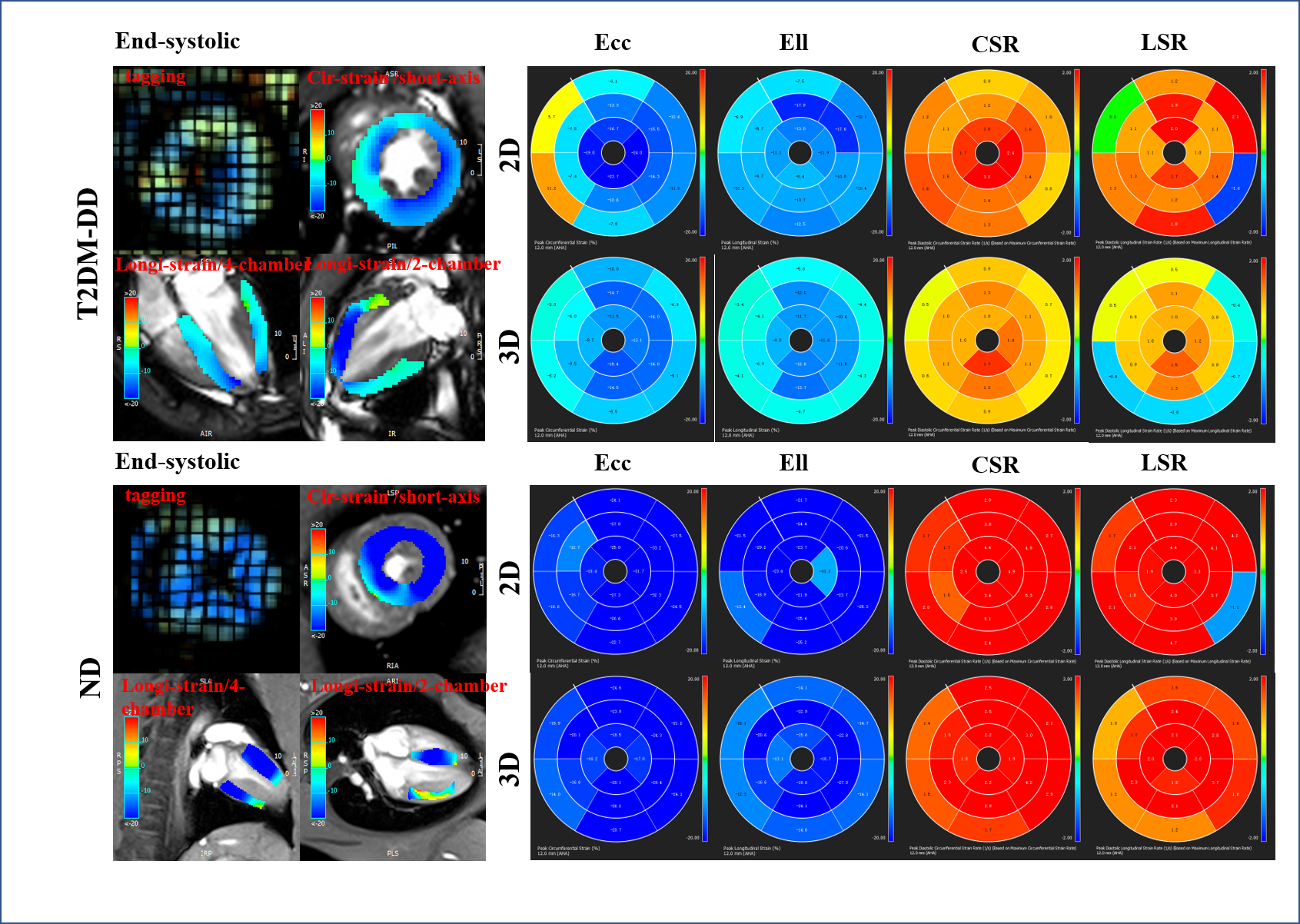
8 spontaneous T2DM rhesus monkeys with isolated diastolic dysfunction (DD) assessed by traditional echocardiography matched with 8 non-diabetic (ND) normal rhesus monkeys were recruited in this study. Cine steady-state free precession were performed in long-axis views and contiguous short-axis slices covering the left ventricle. Short and long-axis tagged images were acquired using a 1-2-1 spatial modulation of magnetization (SPAMM) gradient-echo sequence. LV global circumferential and longitudinal peak systolic strain (Ecc, Ell), and peak diastolic strain rate (CSR, LSR) were assessed using tissue tracking (cmr42, Canada) and an in-house MATLAB HARP analysis tools (Math Works, USA). All CMR imaging protocols was executed twice (i.e. test and retest scans) in 8 ND animals. All systolic and diastolic parameters expressed as absolute value.Results
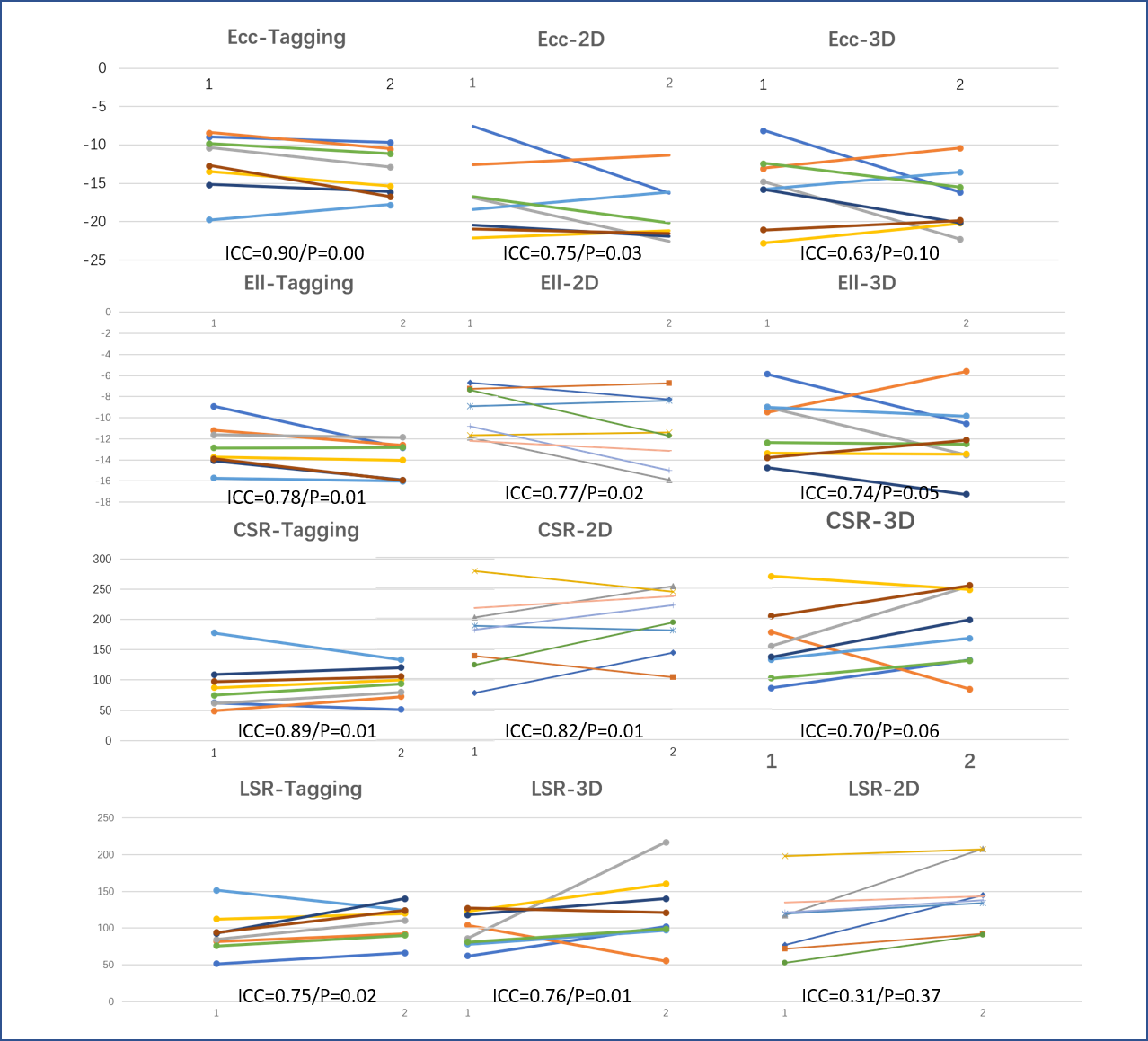
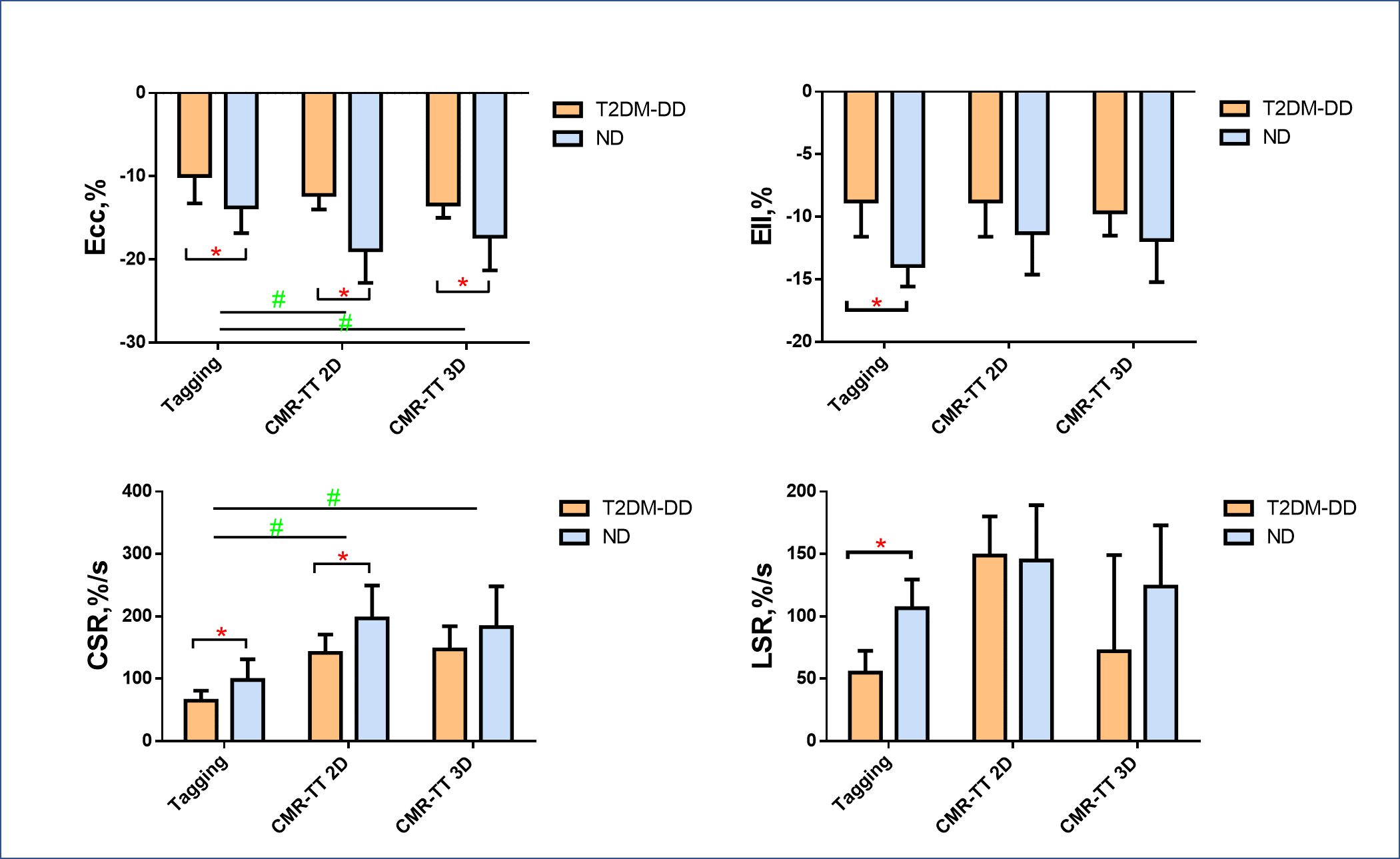
Good test-retest repeatability was observed for all tagging derived systolic and diastolic deformation parameters (shown in the first column of fig.1) which all decreased significantly in T2DM-DD compared with ND(shown in fig.2). CMR-TT derived circumferential systolic and diastolic parameters (Ecc, CSR) were higher measured than tagging, but no obvious difference were found about longitudinal parameters (Ell, LSR)(shown in fig.2). The test-retest repeatability of CMR-TT 3D algorithm derived parameters were lower compared with 2D algorithm result (shown in the second and third columns of fig.2). Thereinto, Ecc had the best correlation with corresponding value of tagging. Comparing the CMR-TT derived parameters between the two groups, we found that CMR-TT 2D derived Ecc, CSR and CMR-TT 3D derived Ecc significantly decreased in T2DM-DD compared with ND (P<0.05) (shown in fig.2).Discussion
The results of CMR strain imaging shown that both systolic and diastolic deformation parameters were reduced significantly in T2DM-DD monkeys which had been diagnosed as isolated early diastolic dysfunction by traditional echocardiography previously. This may reveal a coexistence of systolic and diastolic dysfunction in the early stage of diabetic cardiomyopathy which may have something to do with methodological limitations of systolic abnormalities’ definition.3 In spite of the test-retest repeatability and sensibility are substantially lower with CMR-TT compared with tagging, CMR-TT are able to reveal coexistence of systolic and diastolic dysfunction in T2DM-DD monkeys just as tagging do. Compared with 3D, CMR-TT 2D has higher sensitivity, test-retest reproducibility and higher correlation with tagging which might related to its curvilinear coordinate system based on the mid-surface of the LV wall that does not generalize to multi-chamber topologies.4Conclusion
In the early pathophysiological process of diabetic cardiomyopathy, there are different severity of diastolic and systolic functional damage. CMR-Tissue Tracking, especially 2D algorithm, is able to implement an effective evaluation of the early stage of diabetic cardiomyopathy and is likely to become a potential preferred quantification method in the early diagnosis of diabetic cardiomyopathy.Acknowledgements
No acknowledgement found.References
1. Enomoto M, Ishizu T, Seo Y, et al. Myocardial dysfunction identified by three-dimensional speckle tracking echocardiography in type 2 diabetes patients relates to complications of microangiopathy. Journal of cardiology. 2016;68:282-7.
2. Ibrahim el SH. Myocardial tagging by cardiovascular magnetic resonance: evolution of techniques--pulse sequences, analysis algorithms, and applications. Journal of cardiovascular magnetic resonance : official journal of the Society for Cardiovascular Magnetic Resonance. 2011;13:36.
3. Yu CM, Lin H, Yang H, et al. Progression of systolic abnormalities in patients with "isolated" diastolic heart failure and diastolic dysfunction. Circulation. 2002;105:1195-201.
4. Bistoquet A, Oshinski J, Skrinjar O. Myocardial deformation recovery from cine MRI using a nearly incompressible biventricular model. Medical image analysis. 2008;12:69-85.
Figures