3319
Volumetric Measurements with Real-Time Imaging for Cardiac Stress MRI1Cardiac Imaging, St. Francis Hospital DeMatteis Center for Research and Education, Greenvale, NY, United States, 2Medicine, Stony Brook University (SUNY), Stony Brook, NY, United States, 3Radiology, Stony Brook University (SUNY), Stony Brook, NY, United States
Synopsis
Cardiac stress MRI is a valuable diagnostic tool for heart disease. However, volumetric measurements are challenging because stress introduces rapid heartbeats and body movements. Real-time MRI is advantageous for this application due to its robustness to motion and ability for ungated imaging during free breathing. Here, we demonstrate an undersampled radial balanced steady state free precession (bSSFP) sequence to acquire real-time cine images at high spatial (1.7 mm) and temporal (40 ms) resolutions, applied in cardiac stress MRI. We show that, compared to standard breath-held bSSFP cine MRI, our technique provides more robust and reliable volumetric measurements.
Introduction
Cardiac stress MRI [1] provides a valuable diagnostic tool for heart diseases. However, volumetric measurements are challenging because stress introduces rapid heartbeats and body movements. Real-time MRI [2] is advantageous for this application due to its robustness to motion and ability for ungated imaging during free breathing. Typically, real time MRI is carried out at a low spatial resolution in order to achieve a suitable temporal resolution. This may lead to image degradation and loss of key image features and biomarkers. We have implemented an undersampled radial balanced steady state free precession (bSSFP) sequence to acquire real-time cine images at high spatial (1.7 mm) and temporal (40 ms) resolutions. In this study, we demonstrate that this real-time radial technique produces more robust volumetric results than standard cine bSSFP applied in cardiac stress MRI.Methods
Six healthy subjects with normal cardiac function were imaged at rest (heart rate ~60 BPM) and during stress (heart rate ~100 BPM). Subjects were stressed using an MR-compatible exercise bicycle (Lode B.V., Groningen, the Netherlands) mounted on the scanner table. Images were acquired during bicycling while the subject was inside the magnet bore. MRI was carried out using a 1.5T Avanto system (Siemens Healthcare, Erlangen, Germany).
Real-time freebreathing images (with no ECG gating) were acquired with our undersampled radial bSSFP sequence which acquired 16 radial spokes, uniformly distributed in k-space, for each cardiac phase. Sequence parameters: FOV 240 mm, TR/TE 2.5/1.25 ms, spatial resolution: 1.7 mm, flip angle: 50-70°, readout bandwidth: 1500 Hz/pixel. Since each cardiac phase was reconstructed from 16 radial lines, the temporal resolution was 40 ms. One short axis midventricular slice was imaged in each subject. Acquisition duration was 10 seconds per slice, and multiple cardiac cycles were acquired by each real-time cine image. The undersampled real-time radial images were reconstructed using the correlation imaging framework [3-5]. All subjects were also imaged with a standard breath-held ECG-gated Cartesian bSSFP cine sequence at the same slice locations. Sequence parameters: FOV: 240-280 mm, TR/TE: 2.5/1.25 ms, spatial resolution: 1.5 mm, flip angle: 50-70°, temporal resolution: 90-100 ms, readout bandwidth: 930 Hz/pixel, parallel imaging: GRAPPA (R=2).
The left ventricular (LV) bloodpool was segmented using a semi-automated algorithm. The slice LV bloodpool volume (V) was normalized to the maximum diastolic volume for each subject. A phase state diagram, (Vt,Vt-1) (where t is the time index), was generated and the normalized stroke volume (SV) was estimated from the maximum distance between the systolic and diastolic phases. The ratio of stress-state to rest-state values was computed and the real-time data was compared to the standard bSSFP data using a t-test.
Results
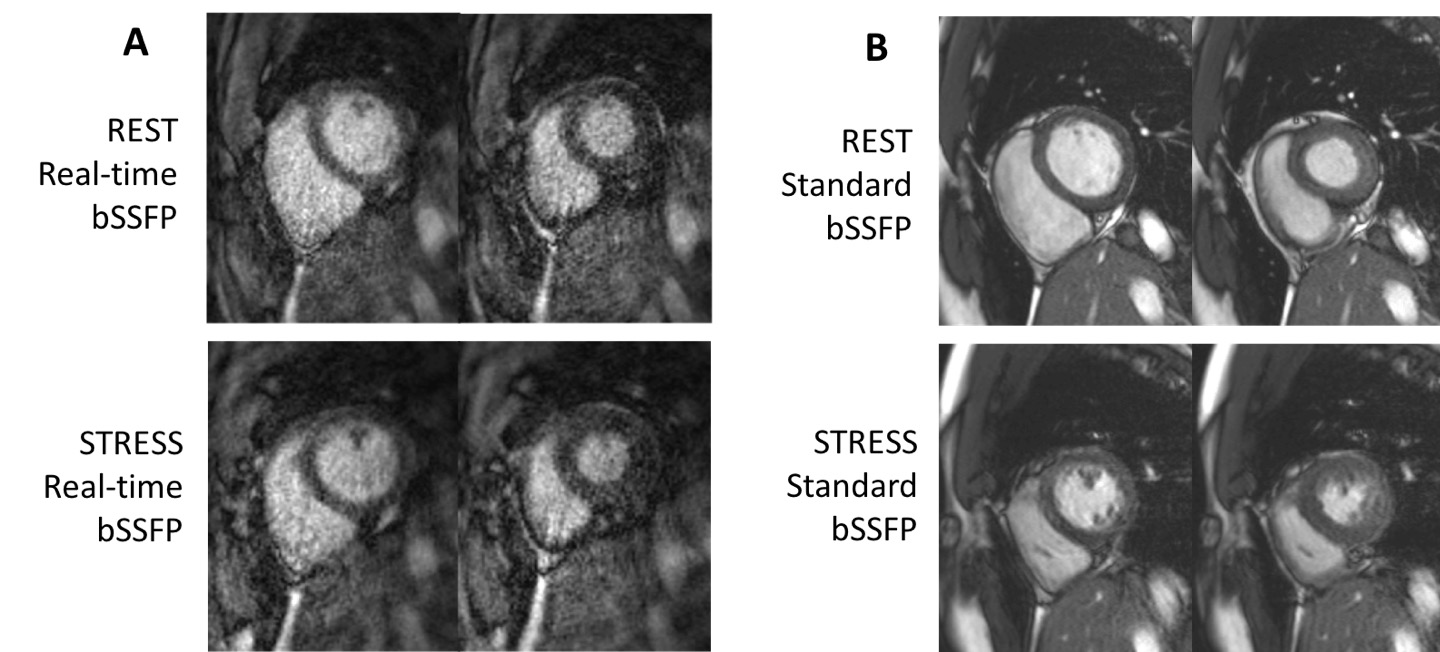
The real-time images for all subjects were reconstructed from the undersampled data. As an example, real-time systolic and diastolic phase images from a subject in rest-state and stress-state are shown in Figure 1A. These images, although reconstructed from only 16 radial lines, provide SNR and spatial resolution comparable to the standard bSSFP cine images (Figure 1B).
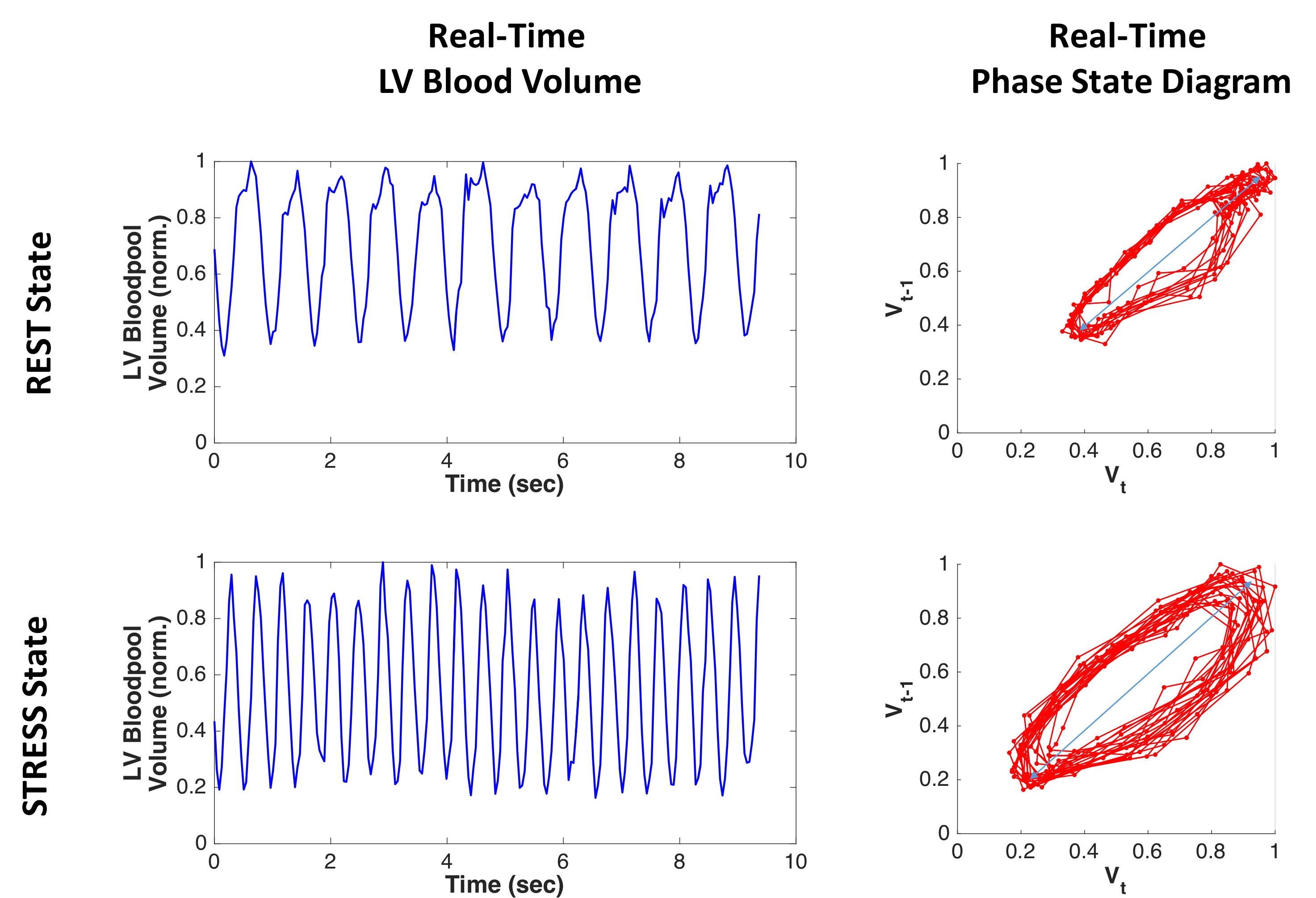
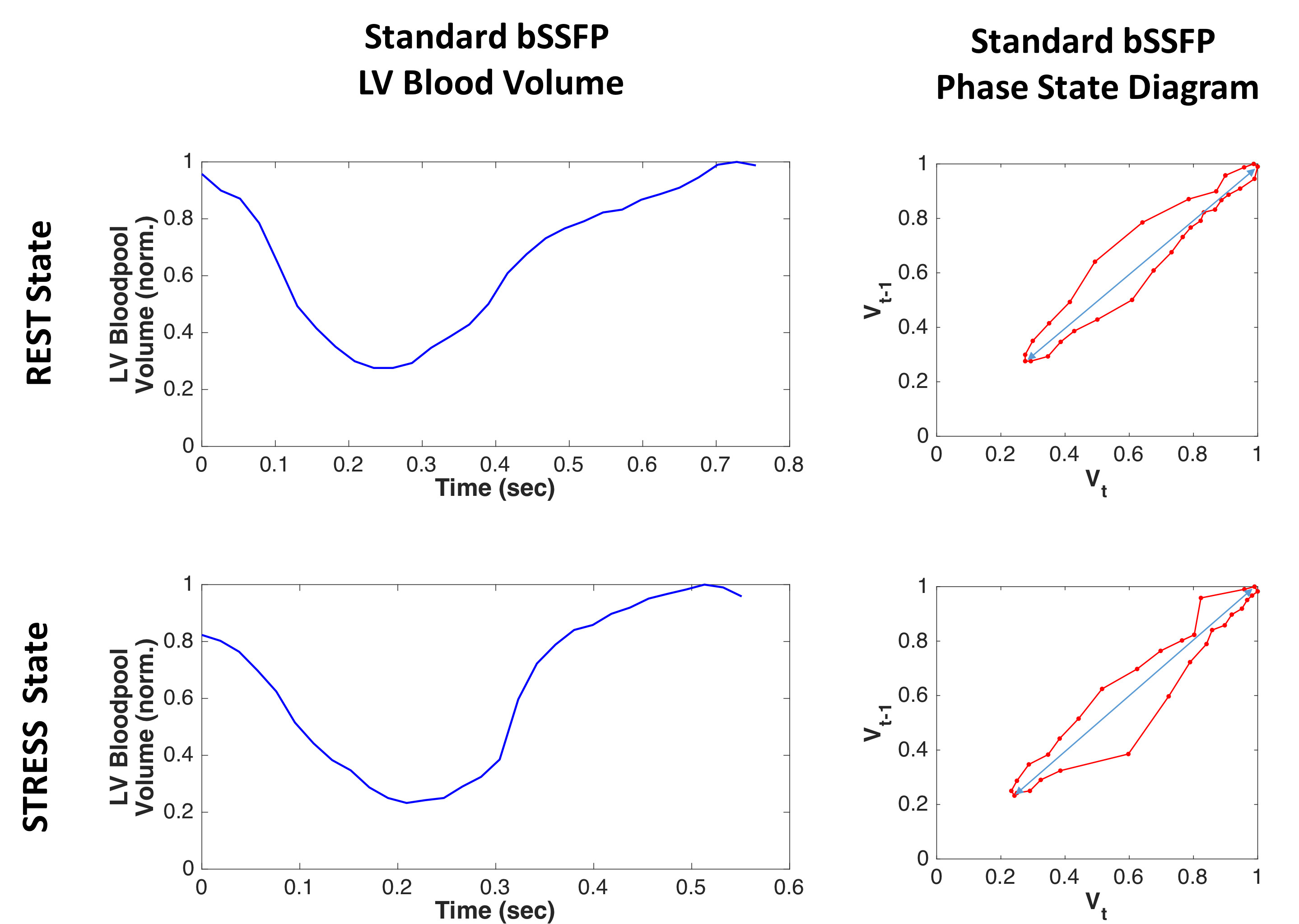
Figure 2 shows the normalized LV bloodpool volume over time for the rest-state and the stress-state for the real-time images for one subject. Respiratory modulation is clearly evident. Also shown are the corresponding phase state diagrams. In comparison, Figure 3 shows these volumetric plots for the standard bSSFP cine images for the same subject.
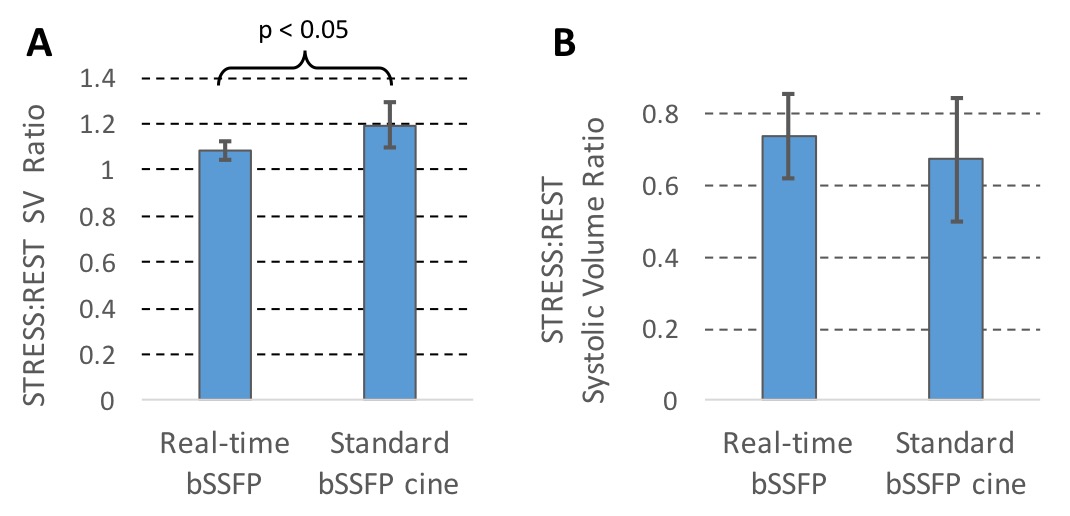
The stress:rest SV ratio for the real-time images was 1.08 ± 0.04, compared to 1.19 ± 0.10 for the standard bSSFP images. These values were significantly different (p < 0.05). The stress:rest systolic volume ratio for the real-time images was 0.74 ± 0.12, compared to 0.67 ± 0.17 for the standard bSSFP images. These values were not significantly different (p > 0.1). These results are depicted in Figure 4.
Discussion
The smaller standard deviations of the real-time volumetric data suggest that the real-time imaging technique is more robust than the standard bSSFP cine imaging. This is reasonable considering that each 2D cardiac phase image in the real-time method is acquired in 40 ms with free-breathing, whereas the standard bSSFP cine is acquired over multiple heart beats during a breath-hold duration. The statistical difference in the stress:rest SV ratio is likely related to respiration (free-breathing vs. breath-holding) and data acquisition (real-time vs. retrospective segmentation). By collecting real-time data in a natural free-breathing state, real-time imaging gives more reliable volumetric measurements for clinical diagnosis.Conclusion
Our proposed real-time cardiac imaging technique is a promising method for cardiac stress MRI and is more robust and reliable compared to standard breath-held bSSFP cine imaging.Acknowledgements
This work is supported by NIH R01EB022405.References
1. Pohost G et al., Circulation 1999, 100: 1676-1679.
2. Basha T et al., MRM 2014, 72(3): 689–698.
3. Li et al., MRM 2012, 68:2005-2017.
4. Li et al., MRM 2015, 74(6): 1574-1586.
5. Li, Proc Intl Soc Mag Reson 2017, 24: 5156.
Figures