3284
Relevance of functional connectivity abnormalities to cognitive impairment in neuromyelitis optica spectrum disodersPaola Valsasina1, Maria A. Rocca1,2, Filippo Savoldi1, Gianna Carla Riccitelli1, Marta Radaelli2, Paolo Preziosa1,2, Giancarlo Comi2, Andrea Falini3, and Massimo Filippi1,2
1Neuroimaging Research Unit, INSPE, Division of Neuroscience, San Raffaele Scientific Institute, Vita-Salute San Raffaele University, Milan, Italy, 2Department of Neurology, San Raffaele Scientific Institute, Vita-Salute San Raffaele University, Milan, Italy, 3Department of Neuroradiology, San Raffaele Scientific Institute, Vita-Salute San Raffaele University, Milan, Italy
Synopsis
In this study, we explored resting state (RS) functional connectivity (FC) abnormalities of the main cognitive networks of patients with neuromyelitis optica spectrum disorders (NMOSD) and their correlation with cognitive impairment (CI). We found increased RS FC in the default mode, salience and working memory networks in cognitively preserved NMOSD, and decreased RS FC in the default mode and working memory networks in CI NMOSD. Increased RS FC seems to contribute to a better cognitive performance, probably reflecting an adaptive mechanism. Conversely, reduced RS FC is likely to be a maladaptive mechanism associated with impaired cognitive functions.
Introduction
Cognitive impairment (CI) is a frequent finding in neuromyelitis optica spectrum disorders (NMOSD) [1]. Aim of this study was to explore resting state (RS) functional connectivity (FC) abnormalities in the main cognitive networks of NMOSD patients.Methods
We acquired RS functional MRI images from 25 NMOSD patients and 30 healthy controls (HC); patients also underwent an extensive neuropsychological evaluation. Patients with at least two abnormal tests (defined as a score more than 2 standard deviations below the normative value) were classified as CI. A cognitive impairment index (CII) was also calculated to evaluate the global extent of cognitive impairment [2]. Independent component analysis (ICA) [3] was performed to identify the main RS networks related to cognition. Between-group comparisons and correlation analysis between RS FC and CII were performed using SPM12 (p<0.001, uncorrected).Results
Nine NMOSD (36%) were CI. CI NMOSD were older (mean age=55.1±6.5 years) compared to CP NMOSD (mean age=36.8±8.4 years) (p<0.001). ICA identified 3 default mode (DMN), 2 salience (SN), 2 executive control (ECN) and 2 working memory (WMN) networks (Figure 1). In the DMN, the NMOSD group and CP NMOSD patients shared higher RS FC vs HC in the precuneus, parahippocampal gyrus and vermis of the cerebellum (Figure 2); the posterior cingulum and the middle occipital gyrus showed higher RS FC vs HC in NMOSD group but lower RS FC vs HC in CI NMOSD (Figure 2). CI NMOSD patients had also lower RS FC vs HC in the cuneus and middle temporal gyrus. In the SN, the NMOSD group and CP NMOSD patients shared higher RS FC vs HC in the supplementary motor area and anterior cingulum (Figure 2). The NMOSD group and CI NMOSD patients shared higher RS FC vs HC in the insula and middle cingulum. In the right WMN, the NMOSD group and CP NMOSD patients shared higher RS FC in the right precentral gyrus (Figure 2). In the left WMN, the NMOSD group and CP NMOSD patients shared lower RS FC in the superior frontal gyrus; the angular gyrus showed lower RS FC vs HC in the NMOSD group but higher RS FC vs HC in CP NMOSD. In the ECN, NMOSD patients showed higher RS FC vs HC in the precuneus. In NMOSD patients, a lower global CII correlated with a lower RS FC in the cuneus of the DMN.Conclusions
Cortical reorganization occurs in NMOSD patients in cognitive RSNs. Increased RS FC contributes to better cognitive performance, probably reflecting an adaptive mechanism. Conversely, reduced RS FC is likely to be a maladaptive mechanism associated with impaired cognitive functions.Acknowledgements
No acknowledgement found.References
[1] Blanc F et al., Arch Neurol 2008; 65: 84-88. [2] Sepulcre J et al., Mult Scler 2006; 12: 187-195. [3] Calhoun V et al., Hum Brain Mapp 2001; 14:140-151.Figures
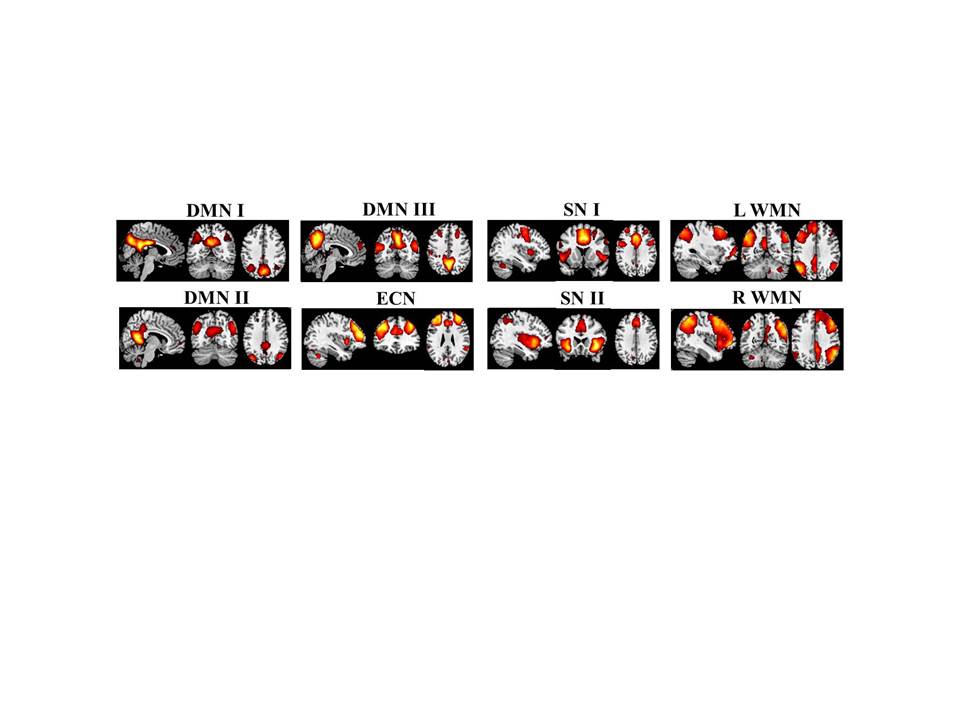
Figure 1. Main cognitive resting state
networks identified by the independent component analysis. Abbreviations:
DMN=default mode network; SN=salience network; WMN=working memory network;
ECN=executive control network; L=left; R=right.
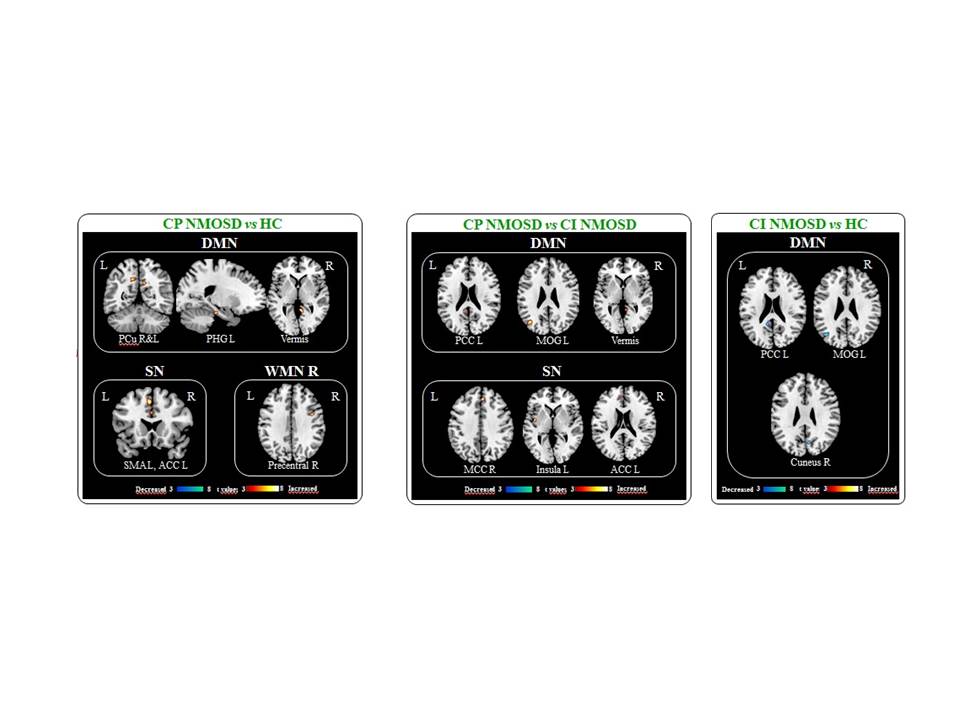
Figure 2. Abnormalities of resting state
functional connectivity detected in cognitively preserved (CP) and cognitively
impaired (CI) patients with neuromyelitis optica spectrum disorder (NMOSD)
compared with healthy controls (HC). Abbreviations: Pcu=precuneus;
PHG=parahippocampal gyrus; SMA=supplementary motor area; ACC=anterior cingulate
cortex; MCC=middle cingulate cortex; PCC=posterior cingulate cortex; MOG=middle
occipital gyrus.