3208
Acute Ankle Sprain: Demonstration of Reliability and Reproducibility of DTI in Imaging Peripheral Nerves1Boston Children's Hospital, Boston, MA, United States, 2University Medical Center Hamburg-Eppendorf, Hamburg, Germany
Synopsis
We investigated potential structural changes in peripheral nerves following ankle sprain injuries. Specifically, we assessed the integrity of the sciatic nerve and its major divisions: the tibial and peroneal nerves. Reduced field-of-view DTI was used, and the reproducibility of the DTI measures was examined. Our results revealed excellent reliability of DTI measures in injured versus control nerves across each parameter (FA, AD, RD, MD). A comparison of injured versus control nerves in the associated nerve branch indicated significant difference in AD. Given these results, DTI may have potential as a powerful tool to determine disease profile.
Introduction
Despite the high prevalence of ankle sprain injuries1, it remains unknown whether peripheral nerves undergo structural changes as a result of injury. As these injuries have been shown to develop into chronic pain syndromes2, this uncertainty may represent lack of consistency or sensitivity in traditional imaging methods. In this investigation, we consider whether DTI can capture reliable metrics with potential use for detecting peripheral nerve changes. As the sciatic nerve innervates the leg, measurement of DTI related changes in this nerve, which encompasses both the tibial and peroneal nerves, could identify if any of these structures are impacted by ankle injuries. A recent publication reported the reliability and reproducibility of peripheral nerve DTI in healthy adult subjects3; however, to our knowledge this method has not yet been employed in a pediatric clinical population. In this study we sought to (1) examine the reproducibility of DTI measures in ankle sprain patients and (2) evaluate the integrity of the sciatic, tibial, and peroneal nerves using reduced field-of-view DTI4.Methods
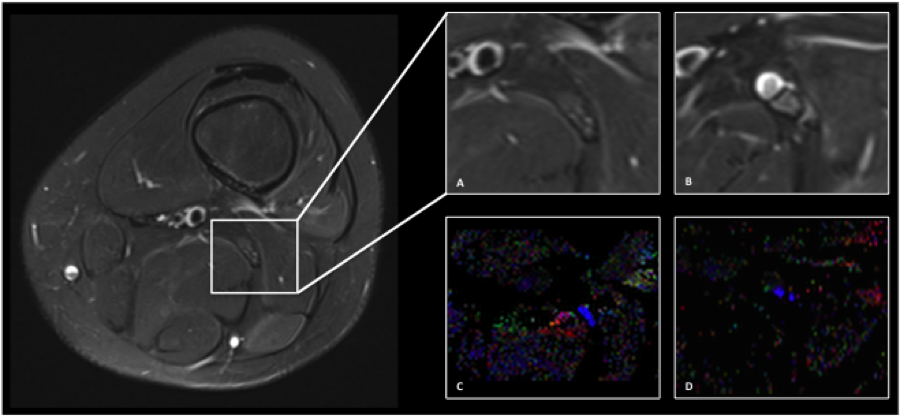
Subjects: 17 patients and 7 controls (mean age= 17 years, range: 11-25) were scanned. Patients had lateral and/or medial ankle injuries. The lateral ankle is innervated by the peroneal nerve, while the medial ankle is innervated by the tibial nerve. The collected values for patients were averaged based on location of injury. Injured nerves were defined as the nerves corresponding to the location of injury (i.e., lateral: sciatic and peroneal; medial: sciatic and tibial). Data acquisition: Subjects were scanned using a 3T MRI system. Sciatic nerve imaging was performed using a 15-Channel knee coil. The imaging protocol included: (1) T2-weighted and (2) reduced-FOV DTI (25 axial slices, FOV=164x47mm2, TR/TE=4400/103ms, 20 diffusion directions, b-value = 750s/mm2, 0.8x0.8x5mm3, averages=4 and acquisition time=7min). Each leg was scanned twice to test for reproducibility of the DTI technique. Data Analysis: DTI data analysis was performed using Olea SphereTM V2.3 (Olea Medical®). The sciatic nerve was localized using T2-weighed images (Figure). Regions of interest were drawn manually at the sciatic, tibial, and peroneal levels on the b0 diffusion images. Fractional anisotropy (FA), mean diffusivity (MD), radial diffusivity (RD), and axial diffusivity (AD) values were reported for each nerve. Results were compared between the injured nerves (patients with ankle sprain) and the healthy controls. Statistical analysis: The Mann-Whitney U test was performed between injured and control nerves for the FA, MD, AD, and RD parameters. Test-retest reproducibility of DTI parameters was calculated using the intraclass correlation coefficient (ICC). Statistical analyses were performed with SPSS V21 (IBM, Armonk, NY). P-value less than 0.05 indicates significant difference.Results
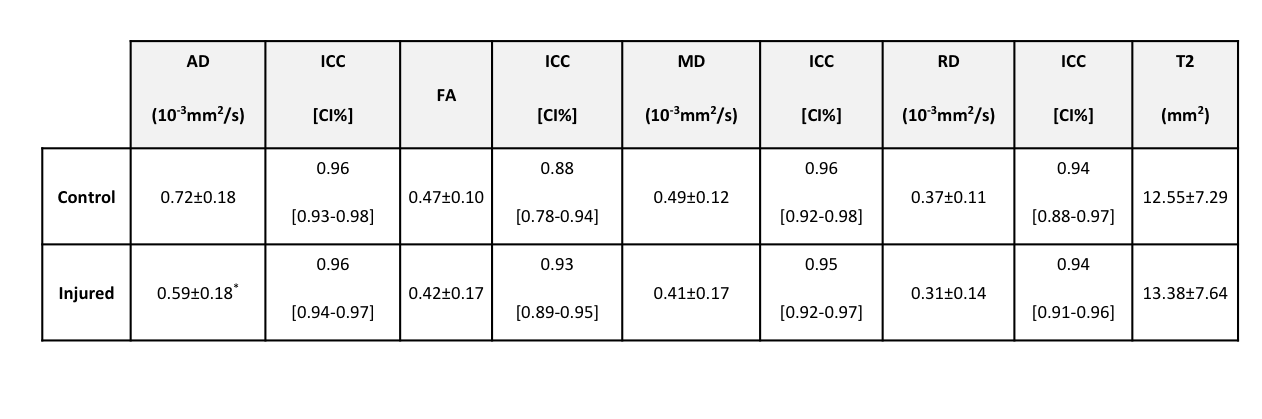
Test-retest analysis revealed excellent reproducibility between the first and second scans: ICC values ranged from 0.88 to 0.98 for AD, FA, RD, and MD in all nerves in both controls and patients (Table). Statistically significant differences were detected in AD values between patients (injured nerves) and healthy controls.Discussion
At present, there exists no conclusive technique to assess structural integrity of peripheral nerves. Given the high frequency with which ankle injuries occur, and their potential to result in chronic pain conditions, a reliable measure to evaluate nerve integrity is urgently needed. This work represents the first application of DTI to measure changes in the sciatic nerve and its branches (tibial and peroneal) in a pediatric clinical model. Test-retest showed excellent reproducibility across DTI parameters and nerves. This finding strongly supports the use of DTI as a reliable tool to detect changes in nerve structure. The significant increases in AD could be attributed to changes in the microstructure of the sciatic nerve and its branches following ankle sprain5. As patients were scanned at the acute phase ( <4 weeks of their injury), the detection of significant structural change so early in the recovery process could also offer support for the high sensitivity of DTI. Future analysis will include longitudinal assessment (i.e. at 3, 6, and 9 months) of nerve damage using DTI and other imaging modalities. Should the DTI parameters continue to demonstrate high reproducibility, in addition to significant differences from controls, the use of DTI should be considered for use as an objective measure of disease profile and treatment efficacy.Acknowledgements
Research reported in this publication was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) of the National Institutes of Health under award number R01, (PI: Borsook).References
1. Waterman BR, Owens BD, Davey S, Zacchilli MA, Belmont PJ, Jr. The epidemiology of ankle sprains in the united states. J Bone Joint Surg Am. 2010;92(13):2279-2284.
2. McBride DJ. Persistent Pain After Ankle Sprain. European Instructional Lectures. 2014. 14:201-209.
3. Simon NG, Lagopoulos J, Gallagher T, Kliot M, Kiernan MC. Peripheral nerve diffusion tensor imaging is reliable and reproducible. J Magn Reson Imaging. 2016;43(4):962-969.
4. Finsterbusch J. Improving the performance of diffusion-weighted inner field-of-view echo-planar imaging based on 2D-selective radiofrequency excitations by tilting the excitation plane. J Magn Reson Imaging. 2012; 35(4):984-992.
5. Basser PJ, Pierpaoli C. Microstructural and physiological features of tissues elucidated by quantitative-diffusion-tensor MRI. J Magn Reson B. 1996; 111(3):209-19.
Figures