3199
Evaluation of cervical cancer staging using readout segmentation of long variable echo-trains and single-shot diffusion weighted echo-planar imaging: a comparison study1Radiology, Suzhou Municipal Hospital, Nanjing Medical University, Suzhou, China, 2Diagnosis Imaging, Siemens Healthcare Ltd, Shanghai, China
Synopsis
Diffusion weighted imaging (DWI) sequence based on readout segmentation of long variable echo-trains (RESOLVE) is superior to that based on single-shot echo-planar imaging (SS-EPI) with respect to improved the image quality, which makes the images more valuable for clinical needs. In this study, we propose an idea to evaluate whether such differences in these images have an impact on staging of cervical cancer. The results show that RESOLVE can improve the accuracy of staging of cervical cancer because of the reductions of image artifacts and geometric deformation.
Background and Purpose
Conventional diffusion weighted imaging (DWI) based on single shot echo planar imaging (SS-EPI) is prone to image artifacts like geometric distortions, image blurring, ghosting artifacts[1-2]. The presence of gas-containing viscera such as rectum and vagina is close to cervical tissue, which results in local field inhomogeneities, and hence, worsen susceptibility artifacts and geometric distortion. All of these may limit its diagnostic value especially in the pelvic. In contrast, readout segmentation of long variable echo-trains (RESOLVE) DWI sequence segments the k-space into several shots along the readout direction in order to shorten the echo spacing, which produces high-resolution DWI images with reduced susceptibility artefact and less blurring arise from T2* signal decay[1.3]. The purpose of our study was to further assess the performance of RESOLVE and SS-EPI in evaluating cervical cancer staging.Methods
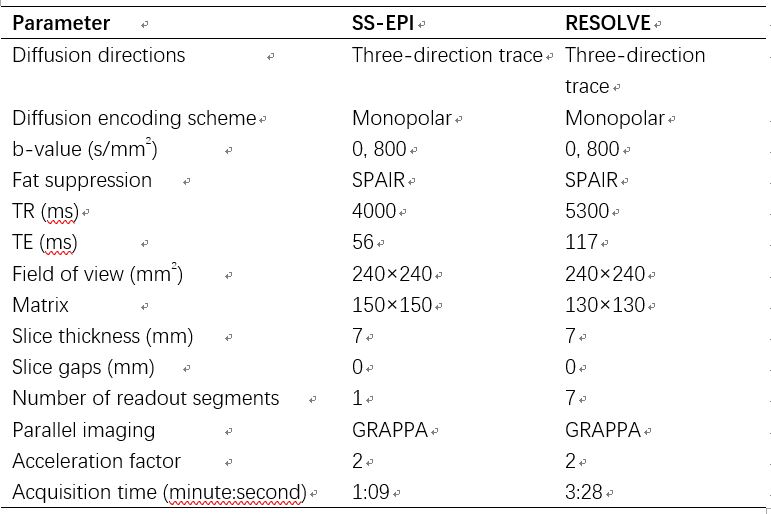
A total number of 61 patients (52±10 years old) with histologically confirmed cervical cancer were involved in this study. MR examinations were performed on a 3 T MR scanner (MAGNETOM Skyra, Siemens Healthcare, Erlangen, Germany) with an 18-channel surface coil in combination with a 32-channel spine coil. Routine examination sequences include axial turbo spin-echo (TSE) T1-weighted imaging, axial and sagittal TSE T2-weighted imaging. Protocols of DWI based on RESOLVE and SS-EPI were listed in Table 1. Two radiologists scored images in terms of distinction of anatomical structures, delineation of lesion, susceptibility artifact and overall diagnostic confidence by using a 4-point scale. The average values of the results from two readers were considered as the final results. Geometric distortion was evaluated by comparing the dimensions of lesions in DWI images with T2WI images. Anterior-posterior (AP) length and left-right (LR) width of the lesions measured on T2WI were used as the dimensional characteristic of the lesion. Staging of cervical cancer on the two DW images were assessed by the two radiologists. Results of cervical cancer staging on SS-EPI and RESOLVE were compared with the gold standard pathological findings.Results
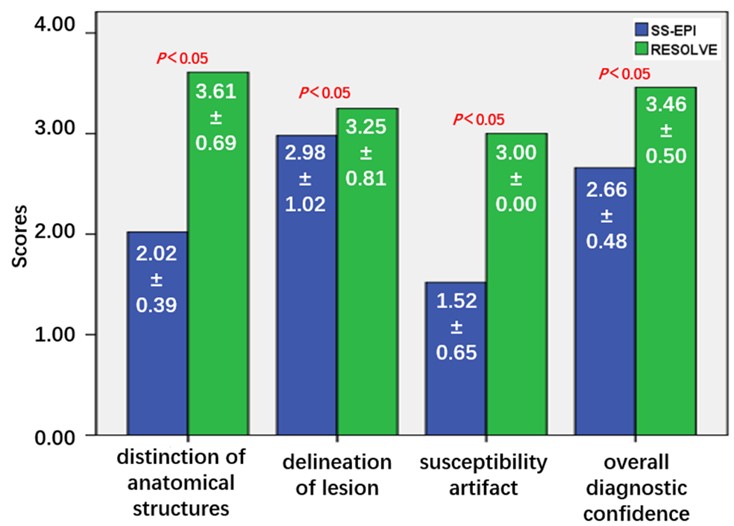
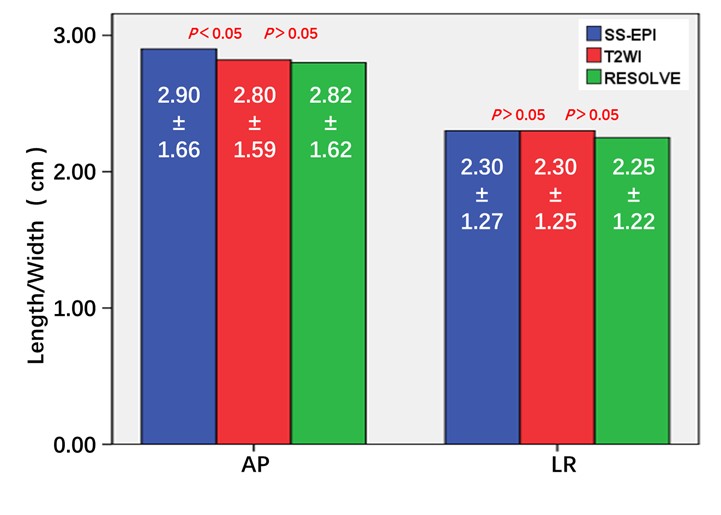
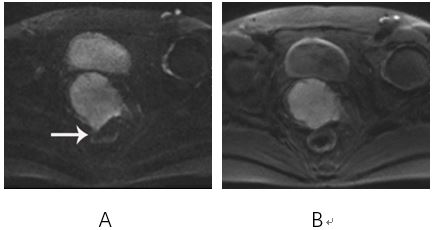
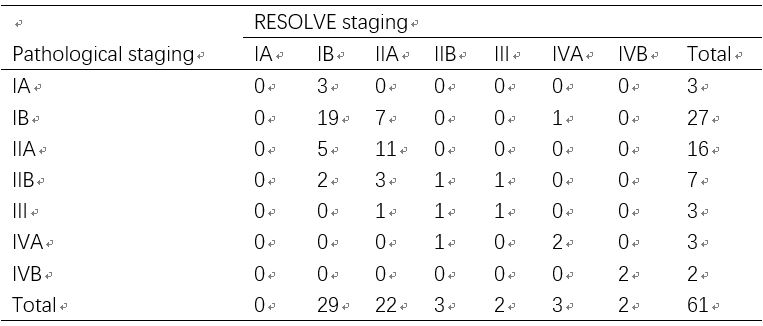
Subjective image quality scores of SS-EPI and RESOLVE is shown in Figure 1. RESOLVE was significantly superior to SS-EPI for all four criteria regarding qualitative comparisons. Comparison of the lesion distortion between DWI (SS-EPI, RESOLVE) and T2WI is shown in Figure 2. There was statistically significant difference in AP between SS-EPI and T2WI. The staging results of pathology, RESOLVE and SS-EPI were respectively listed in Table 2-3. RESOLVE (Z=-1.414, P=0.157) has a better consistency with pathological staging than SS-EPI (Z=-7.227, P=0.000) in staging of cervical cancer. The staging of SS-EPI was overestimated (Figure 3).Discussion and Conclusion
Our study showed that DWI based on RESOLVE has a better performance than that based on SS-EPI as expressed qualitatively for distinction of anatomical structures, delineation of lesion, susceptibility artifact and overall diagnostic confidence in evaluating cervical cancer. The geometric distortion of the lesion was also found to be more severe on SS-EPI. RESOLVE reduces spatial distortion and image blurring by reducing echo spacing and segmenting the readout direction in a contiguous motion compensated multi-shot acquisition[1], which results in better image quality in our study as well as in others’ finding[4]. The unclear anatomical structures, serious artifacts and severe geometric distortion of SS-EPI made the lesions and adjacent normal organs (like parametrial tissue, rectum) boundary unclear, leading to excessive staging. Because of the improvement of RESOLVE in these aspects, the lesions and normal anatomical structures can be clearly displayed, resulting in better staging accuracy. As a conclusion, our study confirmed that RESOLVE is superior to SS-EPI in the accuracy of staging of cervical cancer because of the improvement in image quality.Acknowledgements
No acknowledgement found.References
1. Porter DA, Heidemann RM. High resolution diffusion weighted imaging using readout segmented echo planar imaging, parallel imaging and a two-dimensional navigator-based reacquisition [J]. Magn Reson Med 2009;62(2):468-75.
2. Bogner W, Pinker-Domenig K, Bickel H, et al. Readout-segmented echo-planar imaging improves the diagnostic performance of diffusion-weighted MR breast examinations at 3.0 T [J]. Radiology 2012;263(1):64-76.
3. Wu CJ, Wang Q, Zhang J, et al. Readout-segmented echo-planar imaging in diffusion-weighted imaging of the kidney: comparison with single-shot echo-planar imaging in image quality [J]. Abdom Radiol (NY) 2016;41(1):100-8.
4. Xu X, Wang Y, Hu H, et al. Readout-segmented echo-planar diffusion-weighted imaging in the assessment of orbital tumors: comparison with conventional single-shot echo-planar imaging in image quality and diagnostic performance [J]. Acta Radiol 2017; 58(12):1457-67.
Figures