3188
Interleaved Multi-Slice Averaged Magnetization Inversion Recovery Acquisitions (imsAMIRA) for Fast Spinal Cord Imaging1Division of Radiological Physics, Dept. of Radiology, University Hospital Basel, Basel, Switzerland, 2Dept. of Biomedical Engineering, University of Basel, Basel, Switzerland
Synopsis
To increase the acquisition efficiency for the averaged magnetization inversion recovery acquisitions (AMIRA) approach for spinal cord imaging, an interleaved multi-slice AMIRA implementation was developed. Utilizing a slice-selective adiabatic inversion pulse with optimized slice thickness, the interleaved multi-slice AMIRA sequence provides spinal cord imaging with the same high gray matter and white matter contrast and very similar image quality like the conventional AMIRA approach, however, in considerably reduced scan times per slice.
Introduction
In the past years several MRI approaches have been developed and investigated that tried to mitigate challenges like motion, fine structures and the low contrast between gray matter (GM) and white matter (WM) in the spinal cord (SC)1,2. A disadvantage of the favorite 2D-PSIR approach3 and the recently developed Averaged Magnetization Inversion Recovery Acquisitions (AMIRA) approach4 is that they are inefficient in terms of signal acquisition: a considerable fraction of the acquisition time is needed for relaxation to generate the desired tissue contrast in the SC. In the following, a first realization for an interleaved multi-slice acquisition within the AMIRA technique is presented (imsAMIRA). Essential prerequisites for a working imsAMIRA approach are examined and the resulting images are compared with the corresponding images of the conventional AMIRA approach.Methods
imsAMIRA sequence
The AMIRA sequence, which is based on a manufacturer supplied cardiovascular MR sequence4, was modified to allow a slice loop within a single repetition time TR (imsAMIRA). The slices are freely rotatable and shiftable within the graphical user interface of the MR system. In the simplest version with a slice interleaving factor of 2, the sequence corresponds to the sketch displayed in Figure 1. As a key concept, the former global, i.e. non-selective, adiabatic inversion pulse was replaced with a slice-selective inversion pulse. Additionally, the slice thickness of the inversion pulse (IR-ST) was programmed as a selectable / free parameter in the user interface. The residual sequence was similar to the basic AMIRA approach4: After each inversion recovery (IR) preparation with TRIR-IR = TRIR,slice1-IR,slice1 = TRIR,slice2-IR,slice2 = 3s for a given slice, a dedicated segmented cine-type balanced steady state free precession (bSSFP) readout followed (Figure 1). Eight sample images with the effective inversion times TIeff = [97; 159; 220; 282; 343; 405; 467; 528]ms were acquired for each slice.
General parameters
Apart from the different slice acquisition schemes and the different inversion pulses, the AMIRA and imsAMIRA sequence parameters were identical. In-plane resolution-dependent sequence parameters were: (1) In-plane resolution = 0.67x0.67mm2, matrix = 192x192, 12 k-space lines per segment, TRbSSFP = 5.13ms, TE = 2.14ms. (2) In-plane resolution = 0.50x0.50mm2, matrix = 256x256, 28% phase oversampling, 11 k-space lines per segment, TRbSSFP = 5.5ms, TE = 2.39ms, averages = 2. (3) In-plane resolution = 0.38x0.38mm2, matrix = 336x336, 10 k-space lines per segment, TRbSSFP = 6.0ms, TE = 2.50ms, averages = 2.
Generally, it was FOV = 128x128mm2, flip angle = 35deg and the slice thickness was either 6mm or 8mm as specified in the respective figure.
Performed measurements
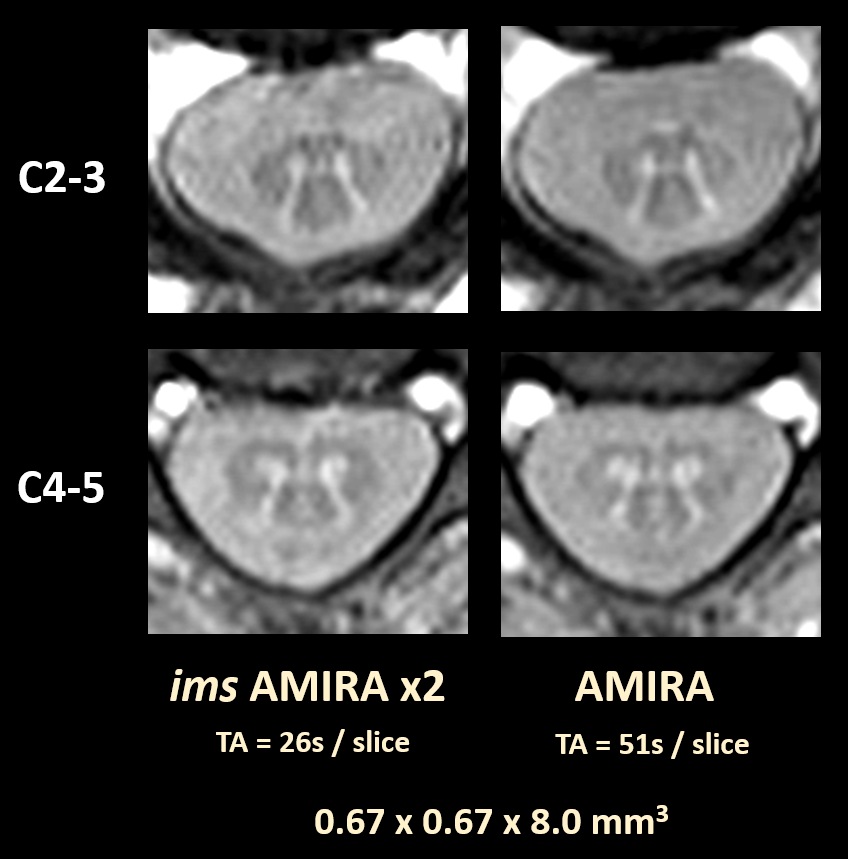
Initially, imsAMIRA experiments were carried out to investigate the optimal slice thickness IR-ST for the inversion pulse. Based on this optimization that had to be done once, comparative measurements between the imsAMIRA and the original (conventional) AMIRA approach were performed. The imsAMIRA sequence acquired two transversal slices simultaneously in an interleaved fashion whereas two separate conventional AMIRA measurements were carried out for comparison (see also Figure 1). Acquisitions were performed at the cervical SC levels C2-3 and C4-5.
All experiments were performed on a 3T whole-body MR system using a 64-channel phased array head and neck coil.
Results
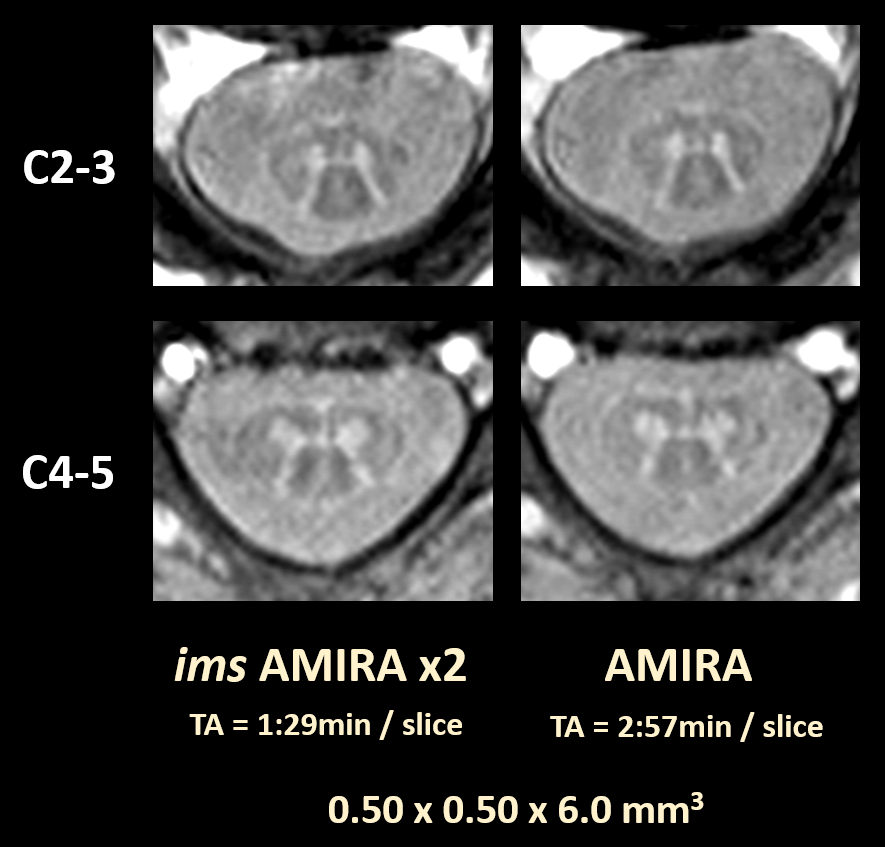
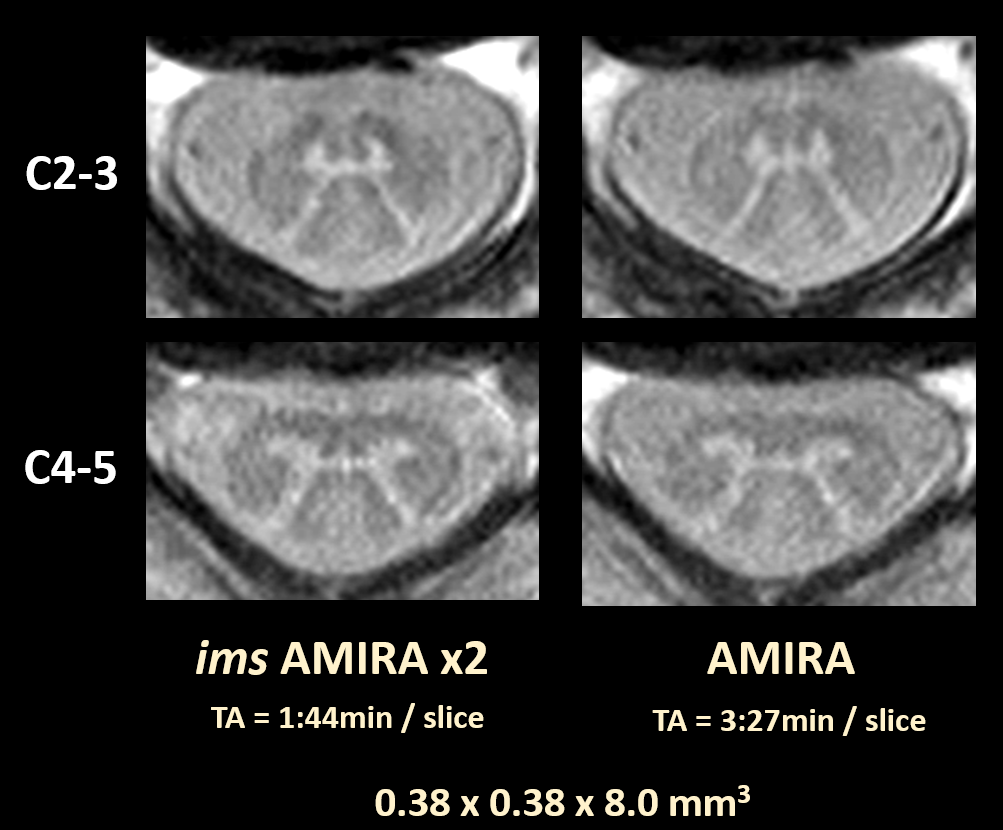
The replacement of the global inversion pulse with a slice-selective inversion pulse causes imsAMIRA to be more sensitive to pulsation effects in the CSF. The suggested solution to this issue is to directly increase the slice thickness IR-ST of the inversion pulse, the resulting effect is illustrated in Figure 2. An increase from the original 2.0x to 4.0x the slice thickness of the bSSFP readout module was found to be sufficient.Figures 3 to 5 present cervical SC measurements of the two approaches with different resolutions. Generally, the imsAMIRA approach demonstrates the same GM-WM contrast and GM-WM structure resolving capability like the conventional single-slice AMIRA approach.
Discussion and Conclusion
The successful implementation of an interleaved two-slice acquisition scheme for the AMIRA approach could be demonstrated (imsAMIRA). Using an optimized inversion pulse slice thickness, potential CSF pulsation artifacts could be mitigated and the suggested imsAMIRA approach provides the same high GM-WM contrast and image quality compared to conventional AMIRA. The increased inversion pulse slice thickness currently limits the minimal gap between the acquired slices in the imsAMIRA approach somewhat, however, already the presented two-slice imsAMIRA approach represents a valuable achievement: The gain of factor 2 in acquisition speed means half the total acquisition time for the whole protocol or the trade for higher signal-to-noise and/or increased resolutions at constant acquisition times.Acknowledgements
This work was funded by the Swiss Multiple Sclerosis Society.References
- Wheeler-Kingshott CA, Stroman PW, Schwab JM et al. The current state-of-the-art of spinal cord imaging: Applications. Neuroimage 2014;84:1082-1093.
- Stroman PW, Wheeler-Kingshott C, Bacon M et al. The current state-of-the-art of spinal cord imaging: Methods. Neuroimage 2014;84:1070-1081.
- Papinutto N, Schlaeger R, Panara V et al. 2D phase-sensitive inversion recovery imaging to measure in vivo spinal cord gray and white matter areas in clinically feasible acquisition times. J Magn Reson Imaging 2015;42:698-708.
- Weigel M, Bieri O. Spinal cord imaging using averaged magnetization inversion recovery acquisitions. Magn Reson Med 2017 Jul 16. doi: 10.1002/mrm.26833.
Figures
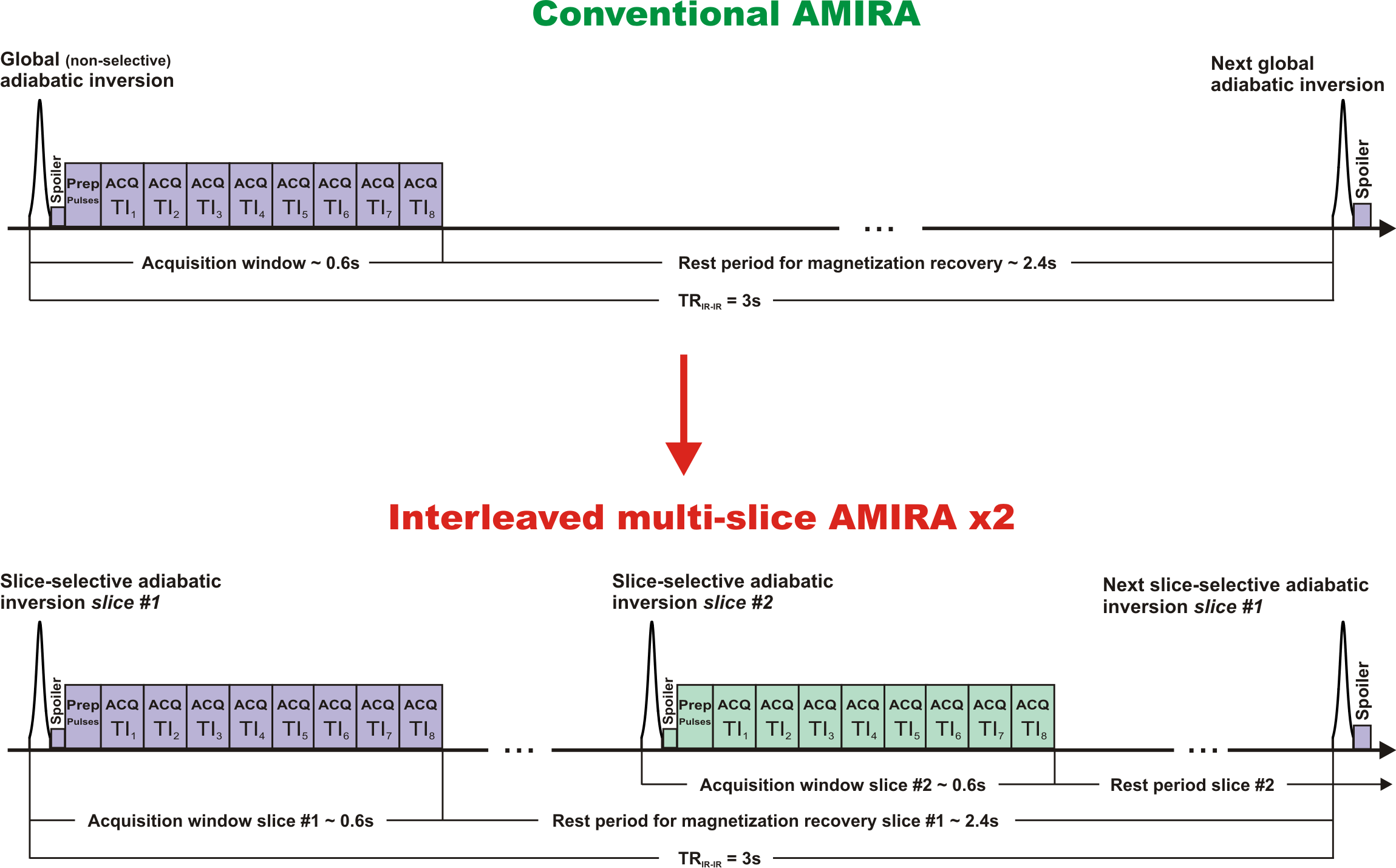
A second key step besides the interleaving of independent slices is the replacement of the global adiabatic inversion pulse with a dedicated slice-selective adiabatic inversion pulse.
Please note that TRIR-IR is defined between consecutive inversion pulses of the same slice.
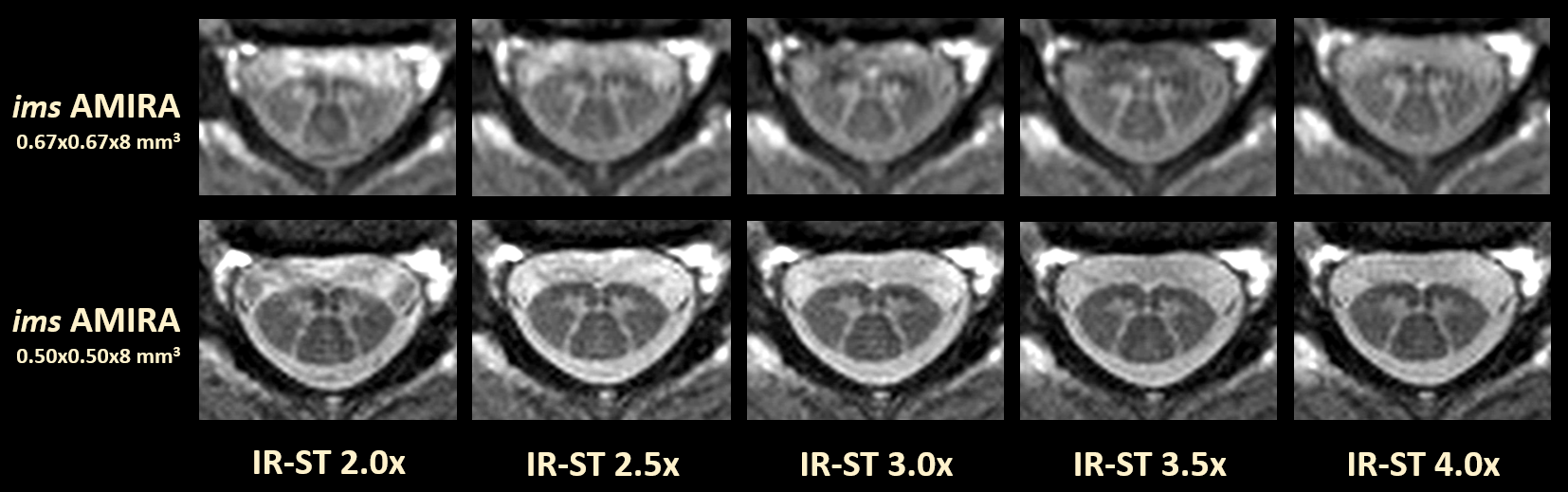
The investigation was performed for two different resolutions as specified.