3086
Positive DTI Findings After Recovery Following Youth Sport-Related Concussion May Be of Little Clinical Relevance1Biomedical Engineering Graduate Program, University of Calgary, Calgary, AB, Canada, 2Paediatrics, Faculty of Medicine, University of Calgary, Calgary, AB, Canada, 3Community Health Science, Cumming School of Medicine, University of Calgary, Calgary, AB, Canada, 4Faculty of Kinesiology, University of Calgary, Calgary, AB, Canada, 5Physicial Medicine & Rehabilitation, Department of Clinical Neurosciences, University of Calgary, Calgary, AB, Canada, 6Department of Radiology, Cumming School of Medicine, University of Calgary, Calgary, AB, Canada, 7Clinical Neurosciences and Psychiatry, University of Calgary, Calgary, AB, Canada
Synopsis
Mild traumatic brain injury (mTBI), including sport-related concussion, is a major health issue. Diffusion Tensor Imaging (DTI) can be useful for identifying alterations in white matter tracts following sport-related concussion. We found that fractional anisotropy (FA) significantly differed between recovered and control youth within the right anterior thalamic radiation and the right inferior longitudinal fasciculus; however, the effect size (< 0.02 change in FA) suggests that the difference may be of little or no clinical relevance, given the recovered group exhibited no symptoms. Large cohort studies are needed before statistically significant MRI findings should be used to inform return-to-play policy
Introduction
Mild traumatic brain injury (mTBI), including sport-related concussion, has become a major health issue. By the age of 25, the lifetime prevalence of a TBI may be as high as 30% and the majority (90%) of cases are of mild severity1. We currently have little knowledge about the impact of concussion on the brain, and what constitutes a “recovered” brain. A recent study using diffusion tensor imaging (DTI) observed reduced diffusivity within some tracts even though patients were clinically recovered, and suggested there may still be injury2. An alternative explanation could be that the DTI observations were of no clinical relevance given the patients were recovered. Thus, it remains unclear what MR findings are of relevance when it comes to recovery following concussion. To help address this issue, in the current study we used DTI to infer structural integrity of white matter tracts in youth hockey players who had recovered from concussion and were recently cleared to play, in comparison to healthy controls
Methods
Thirty youth hockey players (15 recovered after concussion and 15 age-, sex- and level-of-play-matched healthy controls with no history of concussion; age range 11-18 years) were recruited. The recovered subjects were scanned within 7 days of being cleared by a physician to return to play (average 38±12 days between concussion and scanning). DTI was performed using a 3 Tesla GE Discovery MR750w (GE Healthcare ,Waukesha, WI) scanner with a 32-channel head coil (32 diffusion directions, three b=0 T2 images, 2.2-mm slice thickness and b=750 for diffusion weighting). All DTI preprocessing and analysis were performed using FSL. Preprocessing involved motion and eddy current correction and brain extraction. Maps of fractional anisotropy (FA), mean diffusivitiy (MD), axial diffusivity (AD) and radial diffusivity (RD) were calculated for each subject using FSL’s dtifit software and fslmaths. FA maps for all subjects were registered to the standard MNI152 brain template. Tract based spatial statistics3 (TBSS) was then used to align each participant’s FA map to a projected skeleton in MNI152 space, which was then applied to the remaining DTI metrics for all four DTI metrics.
A whole brain voxel-by-voxel analysis was performed between groups for each metric, using FSL’s general linear model approach with the randomise option to correct for multiple comparisons. Using standard white matter atlases (JHU atlases, FSL), 17 major tracts/ROIs were identified, and the mean of each DTI metric was computed for each ROI for each participant, and subsequently tested between groups using a Student t-test.
Results and Discussion
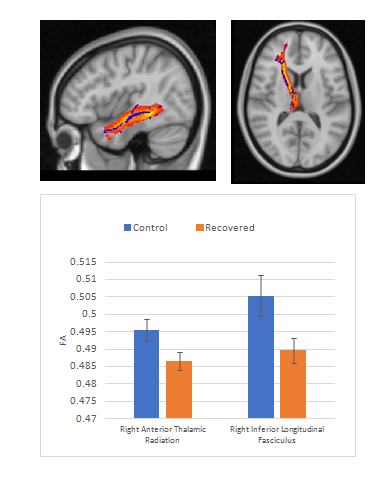
No group difference was observed for the whole brain voxel-by-voxel analysis, suggesting no common site where a DTI metric may have differed between the recovered and control groups. FA significantly differed between the recovered and control youth in the right anterior thalamic radiation and the right inferior longitudinal fasciculus (Figure 1). The remaining DTI metrics (MD, AD, RD) did not differ between groups for any tract/ROI. It is possible that the group difference in FA could indicate residual axonal injury in the recovered group. However, the magnitude of the FA difference between the groups (<0.02) suggests that a more likely explanation that this difference may be a minor compensatory effect that is of no relevance clinically, given the absence of any symptoms.
Conclusion
Sport-related concussion and return-to-play policy are major health and economic issues. While MRI has the power to detect subtle differences between concussed, recovered and control groups, our results demonstrate that these differences need to be considered in the context of clinical relevance. Large cohort studies are needed before statistically significant MRI findings can be used to inform return-to-play policyAcknowledgements
We acknowledge the support of the Canadian Institutes of Health Research, Alberta Innovates Health Solutions, and the Alberta Children’s Hospital Foundation (Vi Riddell Pediatric Rehabiltation Research Program and Integrated Concussion Research Program). The Sport Injury Prevention Research Centre at University of Calgary is one of ten International Olympic Committee Research Centres for Injury and Illness Prevention and Protection of the Athlete. Thank you to the players, parents, coaches, and Hockey Calgary for your support and shared vision in evidence-informed prevention and management of concussions in youth ice hockey players.References
1. McKinlay A, et al. Prevalence of traumatic brain injury among children, adolescents and young adults: prospective evidence from a birth cohort. Brain Inj. 2008 Feb; 22(2):175-81
2. Manning, KY et al. Multiparametric MRI changes persist beyond recovery in concussed adolescent hockey players. Neurology, 2017, epub ahead of print.
3. S.M. Smith, M. Jenkinson, H. Johansen-Berg, D. Rueckert, T.E. Nichols, C.E. Mackay, K.E. Watkins, O. Ciccarelli, M.Z. Cader, P.M. Matthews, and T.E.J. Behrens. Tract-based spatial statistics: Voxelwise analysis of multi-subject diffusion data. NeuroImage.2006; 31:1487-1505.
Figures