3000
Wideband Inversion Recovery Late Gadolinium Enhancement Sequence improves Image Quality in Patients with Cardiac Implanted Electronic Devices1Radiology, Michigan Medicine, Ann Arbor, MI, United States, 2University of Michigan Medical School, Ann Arbor, MI, United States, 3Radiology, University of Michigan, Ann Arbor, MI, United States, 4Cardiovascular Medicine, Michigan Medicine, Ann Arbor, MI, United States
Synopsis
Late gadolinium enhancement is a gold standard for myocardial scar assessment in patients with ventricular tachycardia before their ablation. The presence of cardiac implantable electronic devices degrade the image quality by producing the hyper signal intensity and make the image non-diagnostic. The modified wideband inversion recovery sequence alleviates these hyper signal intensity artifacts and render diagnostic images.
INTRODUCTION
Late gadolinium enhancement (LGE) Cardiac Magnetic Resonance (CMR) is the gold standard for imaging myocardial scar especially in patients with ventricular tachycardia (VT) before ablation procedure [1,2]. The location and the size of the myocardial LGE are instrumental in guiding ablation approach [1]. However, majority of these patients safely undergo CMR despite the presence of cardiac implanted electronic devices (CIEDs) [2-4] which make the LGE imaging challenging because of device-generated metal hyper-enhancement artifacts [1,5]. These artifacts compromise the effect of the inversion recovery (IR) pulse used in the LGE sequence and obscure the region of interest rendering a non-diagnostic image for scar evaluation [1]. An optimized LGE CMR sequence may alleviate the degree of the artifact on the myocardium and allow for visualization of the size and the extent of myocardial LGE. In this study, we determine the fidelity of a modified wideband IR technique as a sequence to alleviate these artifacts and improve the visualization of the myocardial scar.METHODS
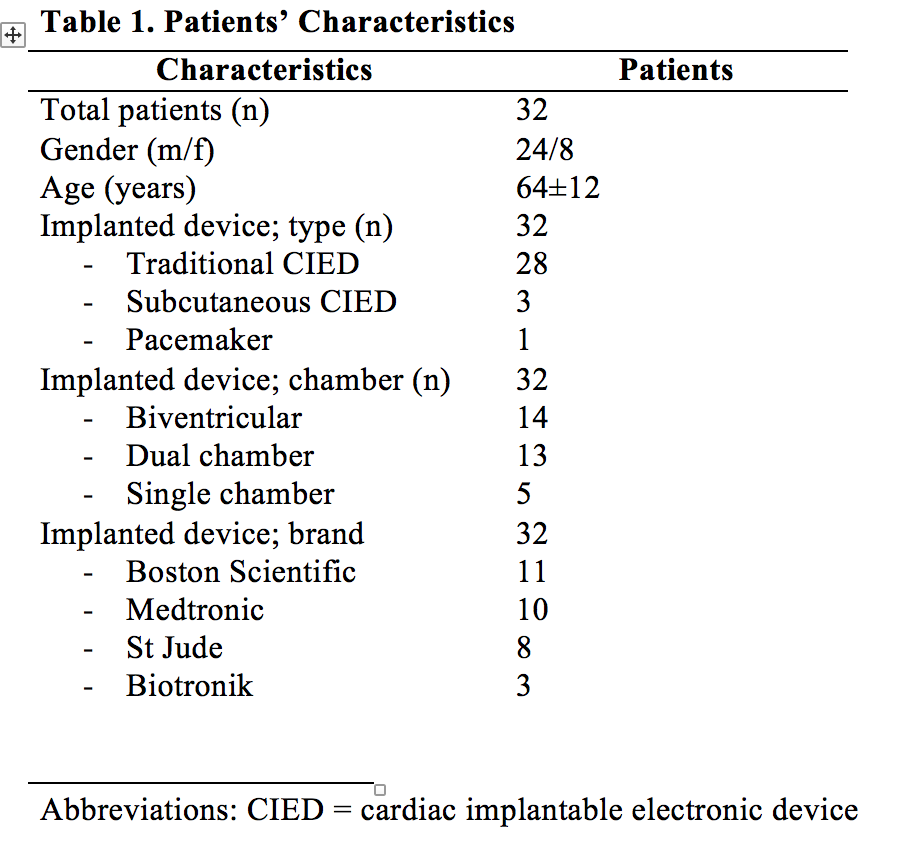
Prior to VT ablation procedures, 32 patients with structural heart disease and CIEDs were scanned on a 1.5T Achieva scanner (Philips, Best, The Netherlands) using both the conventional and modified wideband LGE techniques for assessment of myocardial scar (Table 1). The protocol followed at our institution for MR imaging of CIED patients is limited to 1.5T scanners, where scans ordering is based on necessity and absence of an alternative imaging modality. The device-related relative contraindications include the presence of abandoned leads, pacemaker dependency, and time to lead implant <6 weeks, with the possibility of the ordering physician to overrule these exclusions. The protocol and pre- and post-MRI assessment included interrogation of baseline device characteristics. The patients’ rhythm and vital signs are monitored while the patient is in the scanner. Cardiac scans are performed to assess the existence of LGE prior to VT ablation procedures. The imaging protocol consists of cine short-axis and long-axis images (SSFP sequence, TR=4.2ms, TE=1.8ms, resolution = 1.4×1.4mm2, slice thickness = 8mm) as well as 2D LGE imaging (inversion recovery sequence, TR=6.7ms, TE=3.2ms, resolution = 1.4×2.2mm2, slice thickness=8mm, SAR limit=2W/Kg). The modified pulse sequence includes a wideband IR RF pulse with adjustable frequency offset and bandwidth, which allows for optimal myocardial signal nulling even in the presence of off-resonance effects due to the implanted devices. A phantom experiment was conducted on a 1.5T Philips scanner, where a CIED was placed one-inch away from a water bottle. A cross-sectional image of the bottle was acquired using conventional and wideband IR sequences with different frequency offset and bandwidth (BW) values. The degree of artifact was scored on a scale from 1 to 4, with 1 being the worst (artifact obscures 100% of the left ventricle) and 4 being the best (artifact obscures 0% of the left ventricle). Descriptive statistics and interclass correlation were used to assess the significance level of p<0.05.
RESULTS
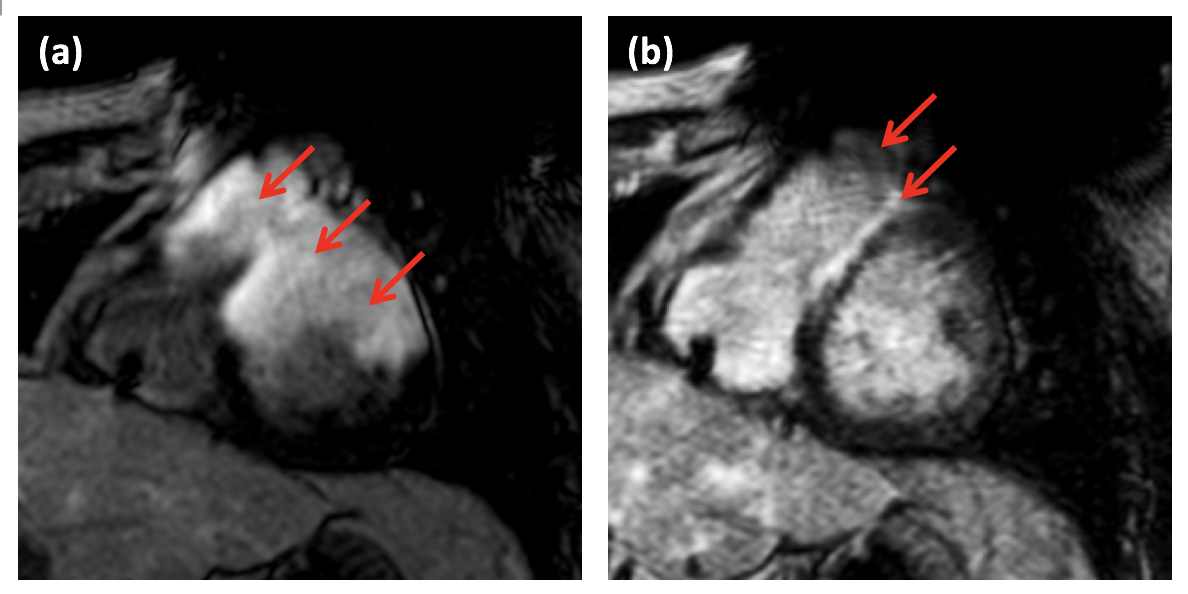
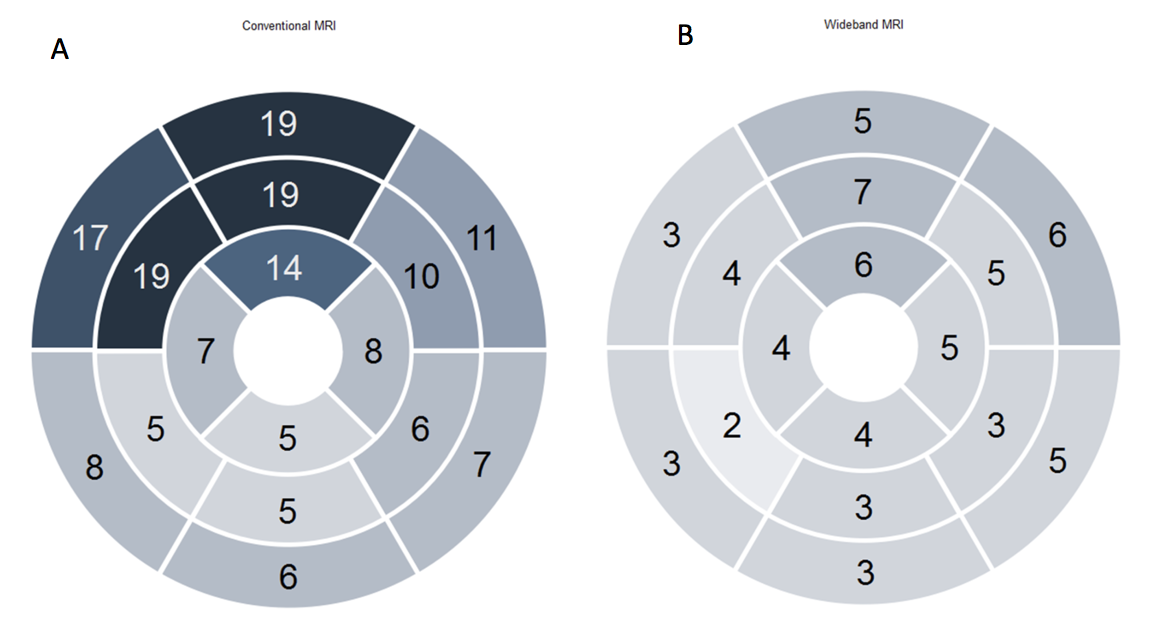
Conventional IR sequence resulted in severe hyper-enhancement artifacts that obscured ventricular segments, making the images non-diagnostic for scar evaluation in 22/32 (69%) of the cases. In the remaining ten (31%) cases, the presence of CIED was not associated with significant hyper-enhancement artifact. The basal and mid anterior and anteroseptal segments were obscured in 19/22 (86%) cases. The wideband IR sequence significantly minimized the artifacts, such that anatomical details could be seen and scar assessment could be confidently performed in 15/22 cases (p<0.0001). In four cases the image quality was improved, but the artifact was still present and in three cases there was no change in the degree of artifact (Figures-1, 2A, and 2B).DISCUSSION
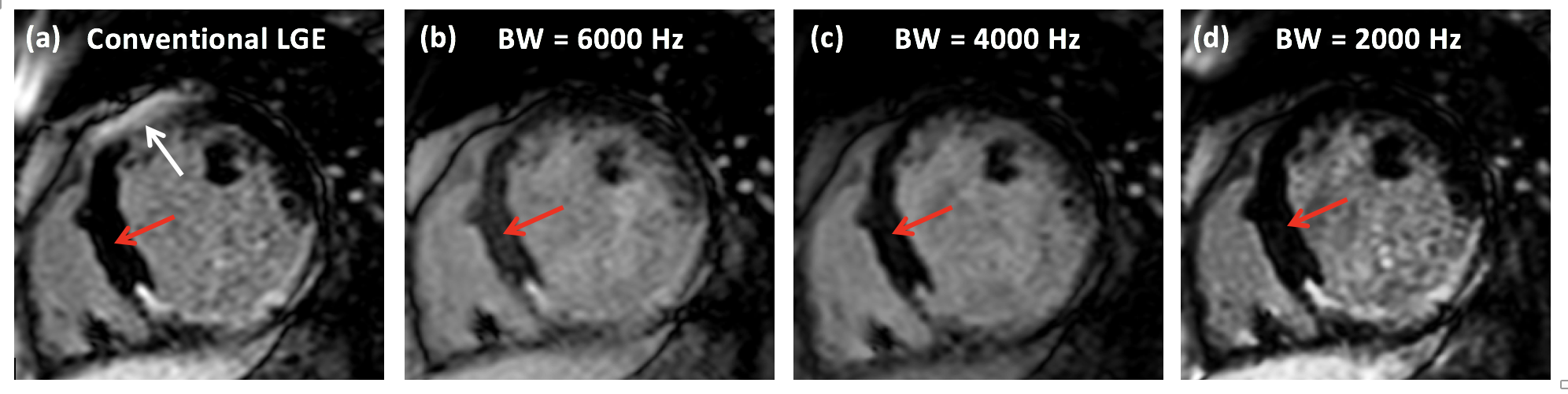
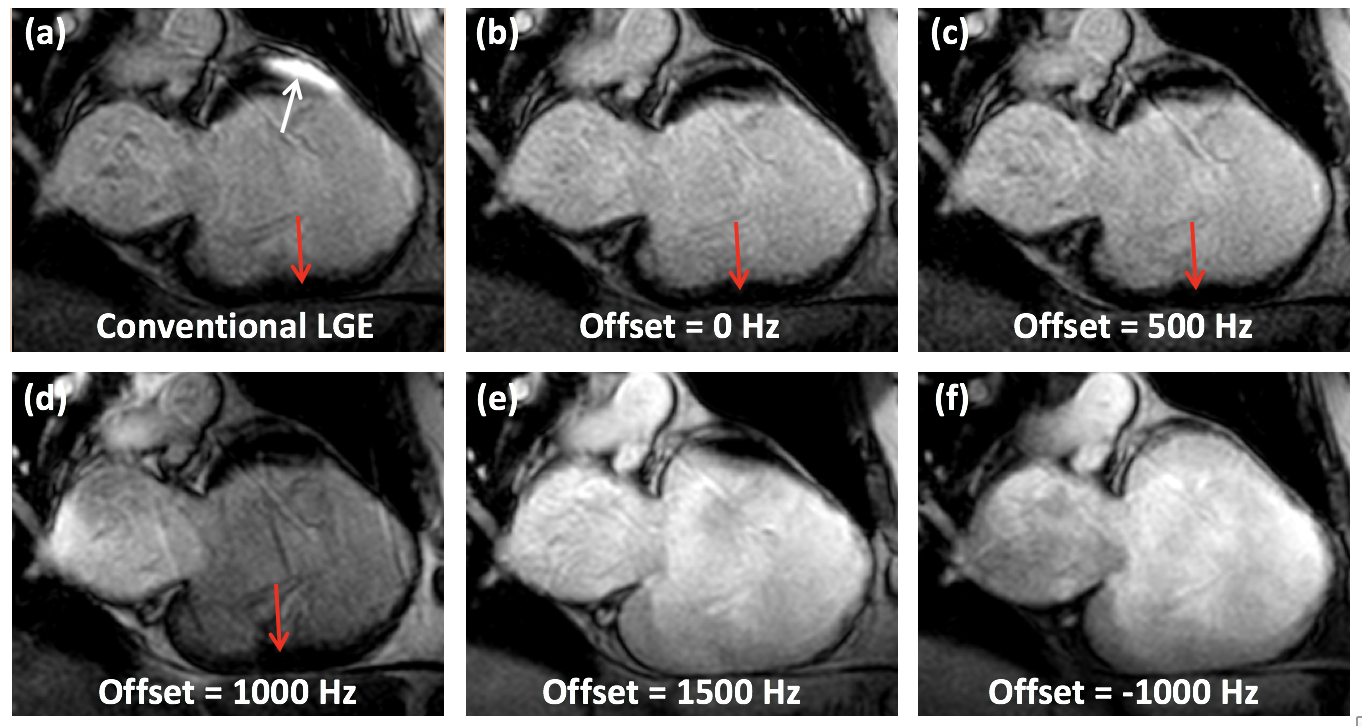
Increasing the IR frequency BW results in better artifact reduction, although this comes at the cost of incomplete myocardial nulling (Figure-3). So, BW should be set to the minimum value that eliminates the artifact, which is affected by the device type and location. Similarly, the frequency offset of the IR pulse affects the artifact appearance (Figure-4), so proper setting of the frequency offset could allow for removing the artifact without the need to increase the frequency BW. Based on the studied cases, optimal BW was in the range of 2000-3000Hz with optimal frequency shift up to 1000Hz.CONCLUSION
The implemented wideband IR technique at 1.5T scanners minimizes the CIED-generated hyper-/hypo-enhancement artifacts without increasing scan time, and allows for accurate identification of arrhythmogenic substrates and ablation targets in VT patients. This study recommends that MR imaging utilizing wideband IR technique be available to more CIED patients who can benefit from it.Acknowledgements
The authors acknowledge the University of Michigan Summer Biomedical Research Program for funding the medical student to work on this project.References
1. Stevens SM, Tung R, Rashid S, et al. Device artifact reduction for magnetic resonance imaging of patients with implantable cardioverter-defibrillators and ventricular tachycardia: Late gadolinium enhancement correlation with electroanatomic mapping. Heart Rhythm, 2014;11(2): 289-298.
2. Nazarian S, Roguin A, Zviman MM, et al., Clinical utility and safety of a protocol for noncardiac and cardiac magnetic resonance imaging of patients with permanent pacemakers and implantable-cardioverter defibrillators at 1.5 tesla. Circulation, 2006;114:1277-84.
3. Nazarian S, Hansford R, Roguin A, et al. A Prospective Evaluation of a Protocol for Magnetic Resonance Imaging of Patients With Implanted Cardiac Devices. Ann Intern Med. 20111;155:415-424.
4. Horwood L, Attili A, Frank L, et al. Magnetic resonance imaging in patients with cardiac implanted electronic devices: focus on contraindications to magnetic resonance imaging protocols, Europace, 2017; 19(5):812-817.
5. Do DH, Eyvazian Y, Bayonets AJ et al. Cardiac magnetic resonance imaging using Wideband sequence in patients with non conditional cardiac implanted electronic devices. Hearth Rhythm 2017;1-8
Figures