2994
Comparison of Whole-Heart Noncontrast-Enhanced 3T MR Angiography and CT Angiography in Detection of Coronary Artery Disease1Peking Union Medical College Hospital, Peking Union Medical College, Chinese Academy of Medical Sciences, Beijing, China, 2Siemens Healthcare, MR Collaborations NE Asia, Beijing, China
Synopsis
The aim of this study was to investigate the diagnostic performance of noncontrast-enhanced coronary MR angiography in the detection of clinical significant coronary artery stenosis by using CTA as a reference. The preliminary results indicate that the noncontrast-enhanced coronary MR angiography has an excellent consistency in evaluating coronary artery disease in comparison to CTA. Noncontrast-enhanced coronary MR angiography may be suitable as a screening tool for coronary artery disease.
INTRODUCTION
Coronary magnetic resonance angiography (MRA) is a promising noninvasive technique for evaluating coronary artery disease(CAD) which allows radiation-free visualization of coronary arteries, and is not affected by the artifacts of severe calcification. The innovative noncontrast-enhanced coronary MRA shows great potential on detecting CAD especially for patients with renal insufficiency, and is a safe technique in a context where contrast agents have raised concerns about deposition in the brain. However, there are less studies in noncontrast-enhanced coronary MRA and lack of large sample literature report especially at 3T MR, compared with enhanced coronary MRA which has demonstrated comparable sensitivity for detectign clinically significant CAD with that of computed tomography angiography (CTA)1. The diagnostic performance of noncontrast-enhanced coronary MRA is still in research. In this preliminary study, we compared the noncontrast-enhanced coronary MRA with CTA for accuracy in the detection of CAD.METHODS
14 consecutive patients with clinically suspected CAD underwent noncontrast-enhanced coronary MRA followed by a CTA scan . All noncontrast-enhanced coronary MRA data were acquired on a MAGNETOM Skyra 3T MR scanner (Siemens Healthcare, Erlangen, Germany). MRA images were acquired using the sequence with the following parameters: TR/TE = 3.3/1.48ms,T2 prep.duration=50ms, FA=20 deg, bandwidth=610Hz/Px, voxel size=0.6x0.6x1.0mm interpolated from 1.2x1.2x2mm3. The CTA examinations were performed at a FORCE 96-row CT scanner (Siemens, Healthcare, Erlangen, Germany) with the following parameters: tube voltage, 100 Kv; tube current, 180 mA; slice thickness 0.75 mm. Contrast agent of 45ml per patient at a rate of 4 ml/s was administered. The quality of the noncontrast-enhanced MRA image was graded for each segment on a four-point scale (1: non-diagnostic, 2: poor, 3: good; 4: excellent). All the segments with quality scored 2–4 and with the diameters larger than 1.5mm were assessed to identify significant narrowing (≥50% lumen diameter reduction) in the comparison with CTA. The inter-modality agreement between MRA and CTA evaluation of coronary artery stenosis was assessed using a Kappa test. SPSS (version 20, IBM, America) was used for data analysis.RESULTS
All 14 patients underwent noncontrast-enhanced MRA successfully with the mean heart beat 68.7 beats per minute (range 49-94bpm). The average imaging time was 11.0±3.4 minutes. A total of 112 segments had a luminal diameter larger than 1.5mm among which 94 (83.9%) segments had a diagnostic image quality and were included in the analysis. The inter-modality evaluation between MRA and CTA was 0.822(p<0.01) representing excellent agreement for assessment of stenosis.DISCUSSION
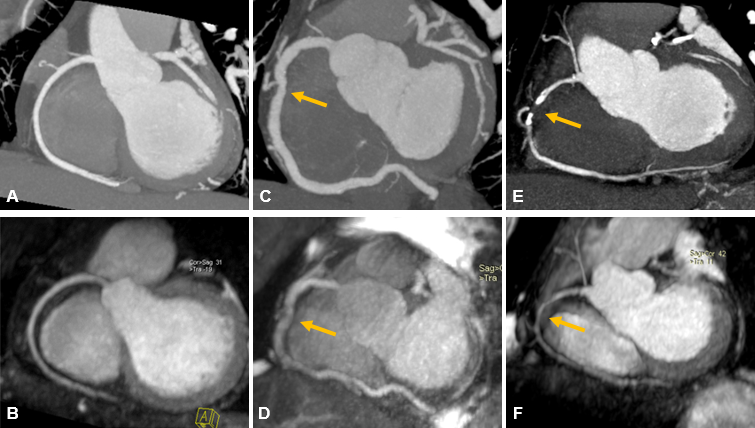
The noncontrast-enhanced coronary MRA showed excellent consistency in detecting CAD with CTA (Figure 1 A-D) indicating a potential alternative that can effectively be used to rule out clinical significate coronary artery stenosis in particular in patients with contraindications to contrast administration. We observed a false negative in our study(Figure 1 E-F). The same result has also been reported in a previous study at 1.5T MR2. One possible reason is that conventional coronary MRA sequences are not flow sensitive and the plaque may contribute to the signal generation. The limitation of this study includes a small sample size and the lack of invasive coronary angiography as gold standard to accurately calculate the diagnostic performance. Further large sample studies and image quality improvements are required.CONCLUSION
Noncontrast-enhanced Whole-Heart coronary 3T MR angiography is a promising noninvasive technique for detecting clinical significant coronary stenosis.Acknowledgements
No acknowledgement found.References
1. Di Leo G, Fisci E, Secchi F, et al. Diagnostic accuracy of magnetic resonance angiography for detection of coronary artery disease: a systematic review and meta-analysis. Eur Radiol. 2016;26(10):3706-3718.
2. Maintz D, Ozgun M, Hoffmeier A, et al. Whole-heart coronary magnetic resonance angiography: value for the detection of coronary artery stenoses in comparison to multislice computed tomography angiography. Acta Radiol. 2007;48(9):967-973.
Figures