2991
Breath Hold Non-contrast Enhanced Angiography of Renal Arteries at 3T using Compressed SENSE Acceleration1Philips Healthcare, Gainesville, FL, United States, 2Radiology, University of Texas Southwestern Medical Center, Dallas, TX, United States, 3Advanced Imaging Research Center, University of Texas Southwestern Medical Center, Dallas, TX, United States, 4Philips Healthcare, Tokyo, Japan, 5MR Resarch & Development, Philips Healthcare, Hamburg, Germany, 6MR Clinical Science, Philips Healthcare, Best, Netherlands, 7MR Resarch & Development, Philips Healthcare, Best, Netherlands
Synopsis
Non-Contrast Enhanced angiography of the renal arteries is an important technology for patients with chronic kidney disease. Existing techniques, like b-TRANCE, have long acquisition times, which makes them sensitive to motion artifacts. Respiratory triggering or navigation can be used to improve motion robustness. This however results in even longer scan times. Compressed SENSE is an effective way for accelerating 3D acquisitions and can be used to substantially reduce scan times. In this study, we report preliminary results of a breath hold and free breathing approaches for contrast-free renal angiography by combining b-TRANCE with compressed SENSE.
Introduction
Non-Contrast Enhanced (NCE) angiography techniques have experienced a resurgence due to safety concerns with gadolinium based contrasts agents and technical advancements in these techniques1. NCE angiography of the renal arteries is especially important for patients with chronic kidney disease. However, many of these techniques suffer from long scan times and are sensitive to artifacts due to breathing motion2. B-TRANCE, a VCG-triggered balanced steady state free precession acquisition in combination with a slice selective inversion pulse, is such a NCE angiography technique3. The acquisition time is normally on the order of 3 to 5 minutes, depending on the required coverage and resolution. In this work, we explore the use of compressed SENSE, the combination of compressed sensing and SENSE, to reduce the acquisition time to fit in a single breath hold. The diagnostic image quality and reproducibility of b-TRANCE of the renal arteries in combination with compressed SENSE was accessed.Methods
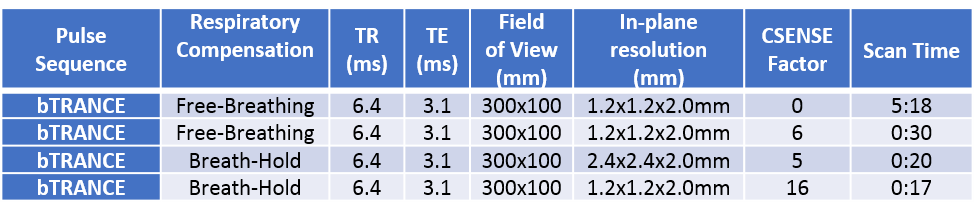
All experiments were performed on a 3T Ingenia Philips MRI scanner (Philips Healthcare, Best, The Netherlands) equipped with a multi-transmit body coil, 16 channel anterior receive coil and 12 channel posterior receive coil. Four normal volunteers underwent scanning to investigate b-TRANCE acquisitions, comparing compressed SENSE acquisitions to standard of care non-accelerated acquisitions, and to investigate the reproducibility of b-TRANCE with compressed SENSE. Acquisition parameters are outlined in Table 1. Two sets of compressed SENSE scans were acquired, one with and one without breath hold. Each b-TRANCE acquisition with compressed SENSE was scanned three times to assess reproducibility. Two additional volunteers were scanned to investigate the utility of b-TRANCE and compressed SENSE at high acceleration factors (up to 16). The compressed SENSE method used is a fully integrated combination of compressed sensing and SENSE, using variable density sampling and sparsity constraint in the wavelet domain. The regularization parameter to balance sparsity constraining and data consistency was set to a level of de-noising of 20%. Images were then reviewed by a radiologist to access image quality, demonstrated diagnostic criteria, and reproducibility. The study adhered to the local Institutional Review Board guidelines.Results
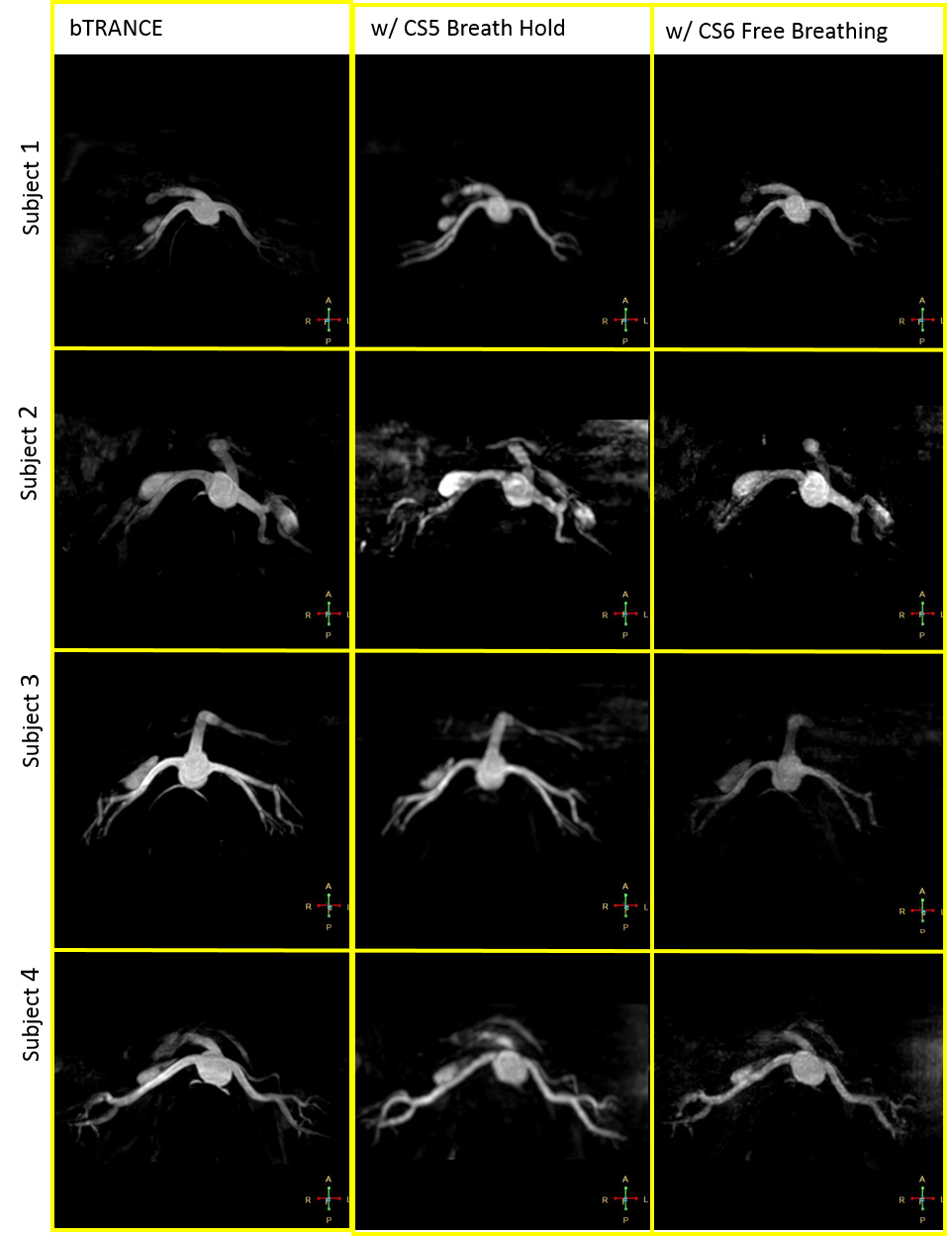
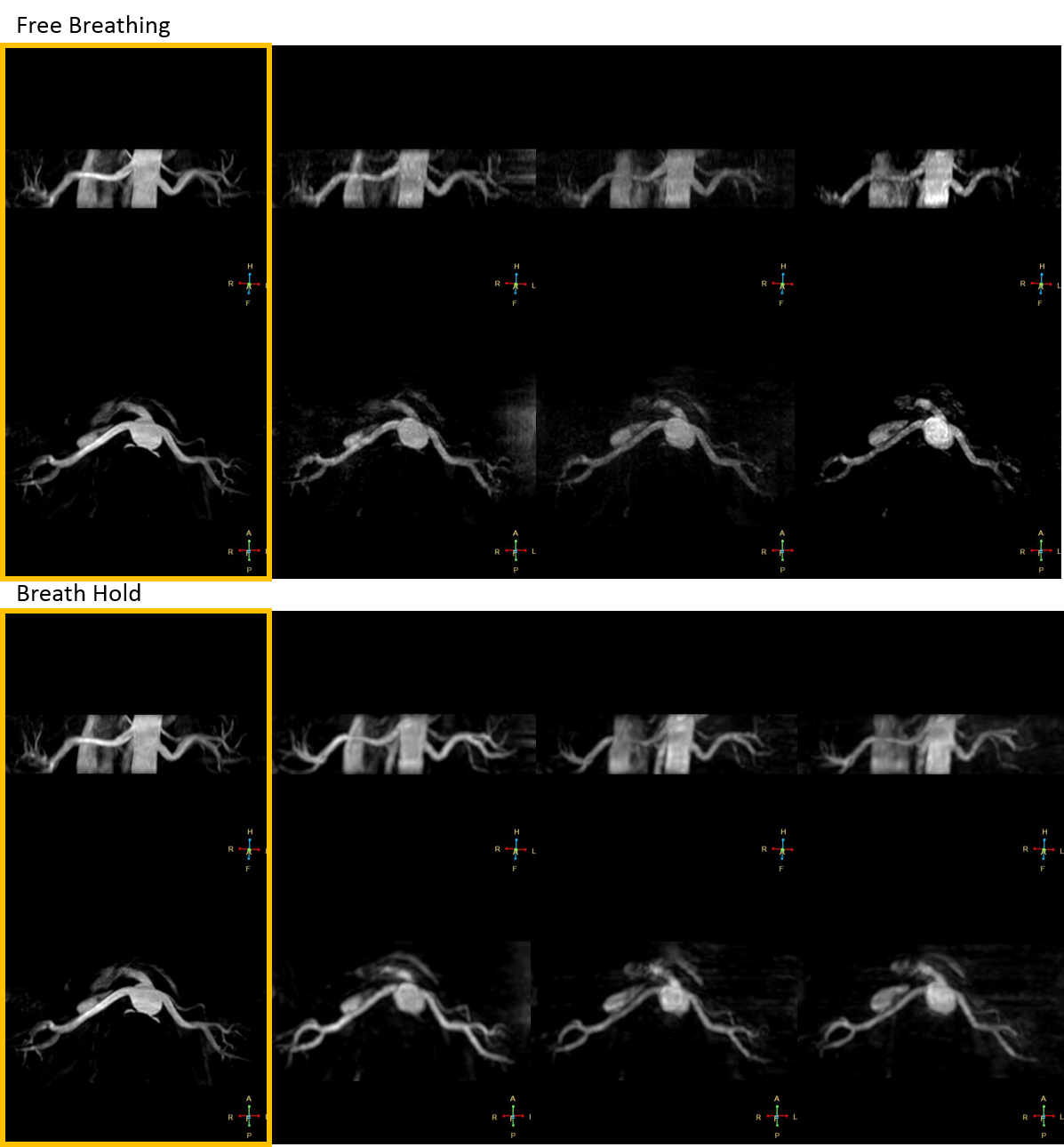
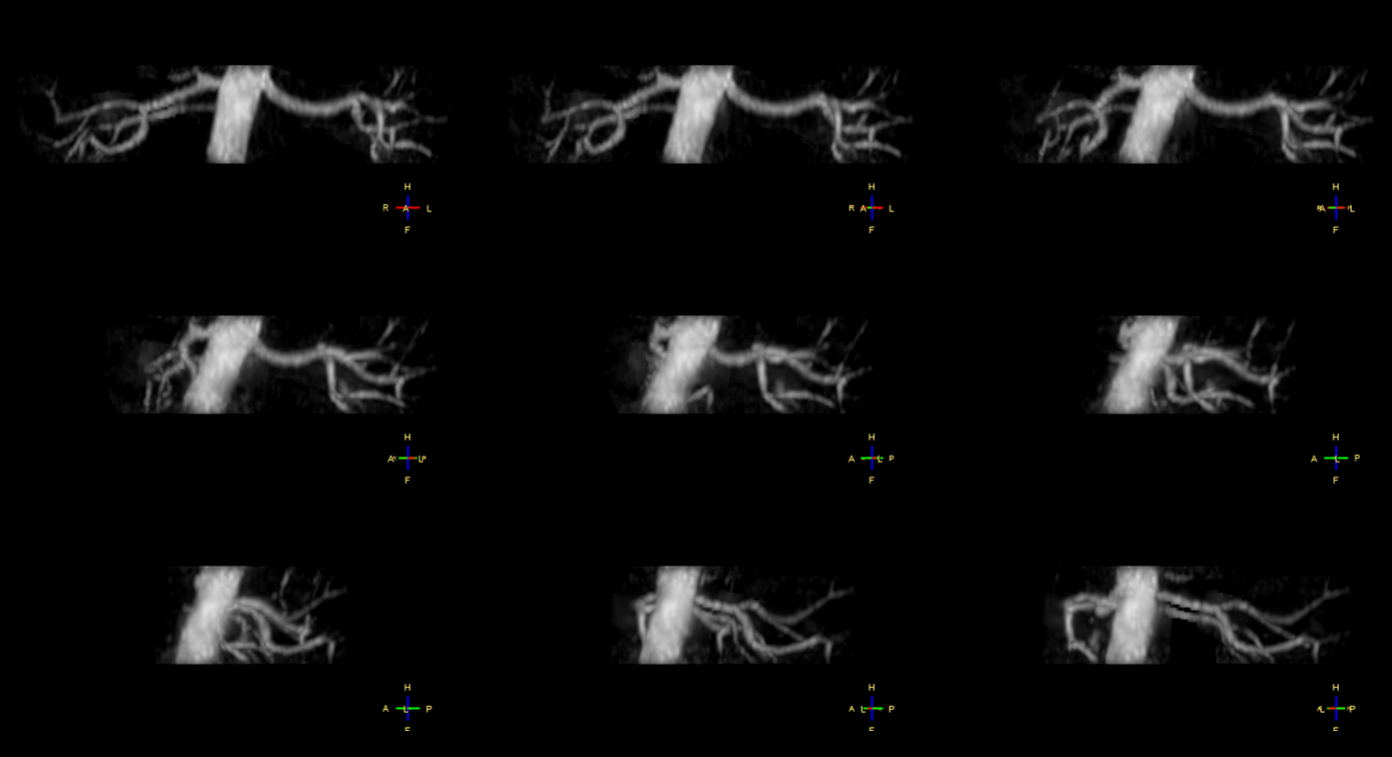
Figure 1 shows representative maximum intensity projections (MIP) of the b-TRANCE acquisitions with compressed SENSE compared to images acquired without any acceleration. Figure 2 shows reproducibility scans from one volunteer for the breath hold and non-breath hold techniques. Figure 3 shows the source and MIP images from one volunteer acquired with an acceleration factor of 16 that resulted in a breath hold time of 19 seconds, while still retaining the resolution of the non- accelerated acquisition. The renal arteries are clearly depicted in all images. Review by a radiologist reported all scans being of diagnostic quality, with high image quality reproducibility.Discussion
Our preliminary results suggest that b-TRANCE with compressed SENSE can provide diagnostic quality images that can be acquired in a single breath hold. Image quality with compressed SENSE was also shown to be consistent and reproducible. b-TRANCE with compressed SENSE allows for a drastic time savings and may lead to routine clinical use without the need to administer contrast. Given that b-TRANCE is currently a non-breath hold technique, we also show that when combined with compressed SENSE it can still be used to acquire a diagnostic renal MRA in 30 seconds. This has direct clinical utility given not all patients can perform consistent breath holds or remain on the table for lengthy scan acquisitions. These overall time savings with both breath hold and non-breath hold techniques will translate to increased productivity.Acknowledgements
No acknowledgement found.References
1.Miyazaki, Mitsue, and Hiroyoshi Isoda. "Non-contrast-enhanced MR angiography of the abdomen." European journal of radiology80.1 (2011): 9-23.
2.Wheaton, Andrew J., and Mitsue Miyazaki. "Non‐contrast enhanced MR angiography: Physical principles." Journal of magnetic resonance imaging 36.2 (2012): 286-304.
3.Maki, Jeffrey H., et al. "Steady‐state free precession MRA of the renal arteries: Breath‐hold and navigator‐gated techniques vs. CE‐MRA." Journal of Magnetic Resonance Imaging 26.4 (2007): 966-973.
Figures