2988
Breath-hold Three-dimensional Quiescent-Interval Slice-Selective (QISS) MR Angiography using a Fast-Interrupted Steady-State (FISS) Readout: Application to the Coronary and Renal Arteries1Radiology, NorthShore University HealthSystem, Evanston, IL, United States, 2Radiology, Feinberg School of Medicine, Northwestern University, Chicago, IL, United States, 3Siemens Medical Solutions, Chicago, IL, United States, 4Radiology, Prtizker School of Medicine, University of Chicago, Chicago, IL, United States
Synopsis
Quiescent-interval slice-selective (QISS) is a robust nonenhanced 2D MRA technique, but has potential limitations regarding minimum slice thickness, slice profile, and fat suppression. We therefore implemented a breath-hold prototype 3D version of QISS which uses a thin-slab RF excitation, stack-of-stars k-space trajectory, and fast interrupted steady-state (FISS) readout instead of bSSFP. 2D and 3D QISS were compared for imaging of the coronary and renal arteries. Benefits of 3D QISS included better depiction of small branch vessels and improved quality for multi-planar reconstructions.
Introduction
Quiescent-interval slice-selective (QISS) using a Cartesian k-space trajectory was originally described for nonenhanced MR angiography (MRA) of the peripheral arteries, but radial variants have since been applied for MRA of the coronary arteries [1] and pulmonary arteries [2]. 2D QISS uses a balanced steady-state free precession (bSSFP) readout, which necessitates minimizing the duration of the radiofrequency (RF) excitation pulse to shorten the echo spacing and reduce the sensitivity to flow and off-resonance artifacts. A short-duration RF pulse in combination with a large flip angle can be problematic for several reasons including: (1) non-rectangular slice profile, so that the effective slice thickness is larger than the nominal thickness; (2) the minimum achievable slice thickness is restricted by the RF pulse duration and peak gradient amplitude to about 2-mm.
To overcome these limitations, we implemented a prototype 3D version of QISS which uses a thin-slab RF excitation and stack-of-stars k-space trajectory. Unlike 2D QISS which uses a bSSFP readout, the 3D QISS technique uses a recently developed fast interrupted steady-state (FISS) readout [3]. 2D QISS and 3D QISS were compared for imaging of the coronary and renal arteries.
Methods
The study was IRB-approved. The coronary and renal arteries were imaged in healthy volunteers using a 1.5 Tesla scanner (MAGNETOM Avanto, Siemens Healthcare, Erlangen, Germany). Images were acquired during a single breath-hold using electrocardiographic gating. 2D and 3D QISS techniques were compared using similar acquisition parameters, including: slice thickness = 2-mm, 96 radial views, 1 or 2 shots, equidistant azimuthal view angles, in-plane field of view ~ 250 – 280-mm, sampling bandwidth ~ 890 Hz/pixel. The FISS readout differs significantly from a conventional bSSFP readout in that the steady-state magnetization undergoes gradient and RF spoiling after each block of 6-8 bSSFP modules.
For both 2D and 3D QISS of the coronary arteries, an in-plane adiabatic inversion RF pulse was applied followed by a quiescent-interval of several hundred msec; a fat saturation RF pulse was only used for 2D QISS. For both 2D and 3D QISS of the renal arteries, two inversion slabs were applied in a V-shape spanning the proximal renal arteries through the kidneys; no fat saturation RF pulse was applied.
Results
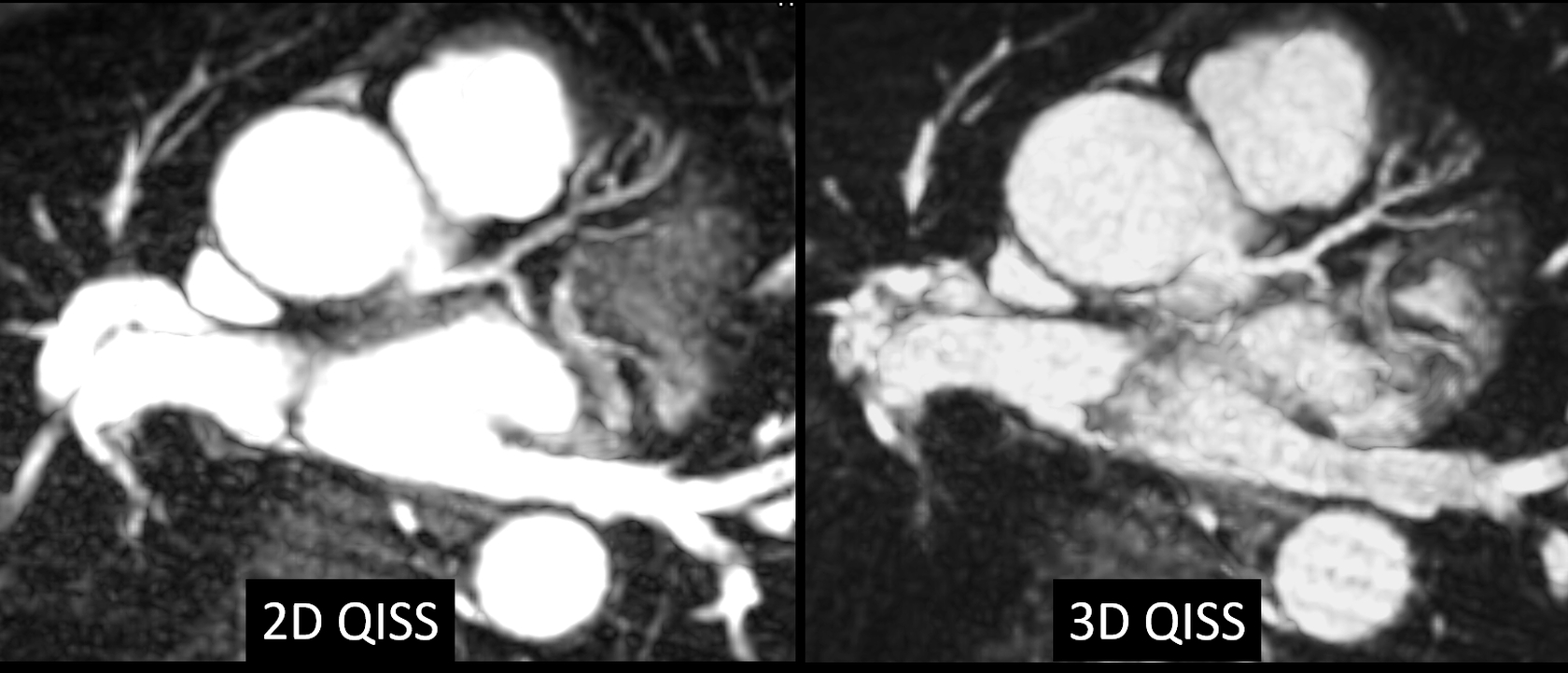
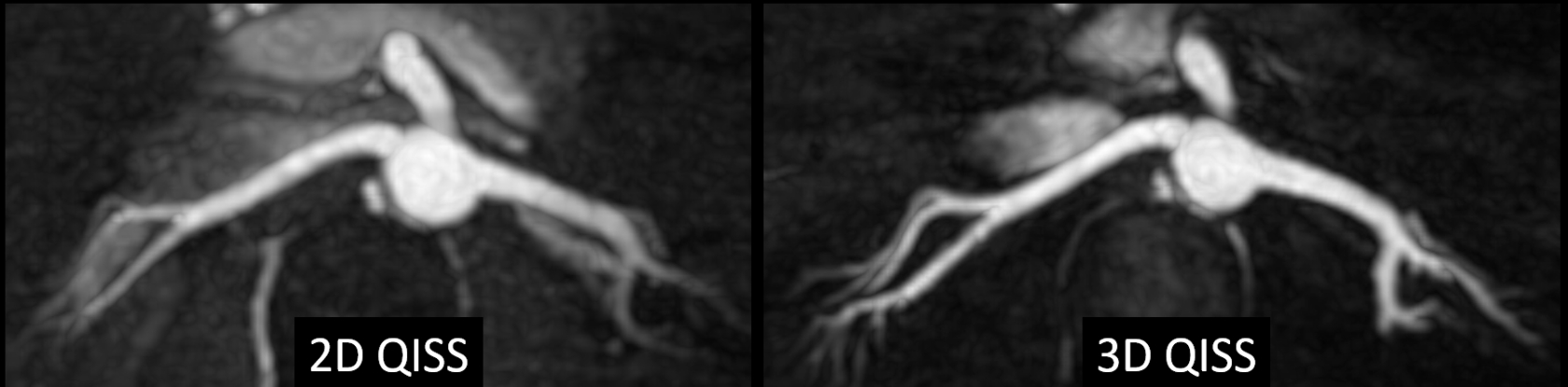
Image quality was generally similar for 2D and 3D QISS. The coronary arteries were reliably demonstrated, and the vessel diameter and visualized length of vessel were similar for the two techniques. Small branch detail and the quality of multi-planar reconstructions were improved with the 3D approach (Figure 1). Comparing 2D and 3D QISS of the renal arteries, the extra-renal portions of the renal arteries appeared similar, whereas intra-renal branches were better depicted with the 3D approach (Figure 2). For coronal acquisitions using 3D (but not 2D) QISS, the slice orientation needed to be tilted to avoid excessive saturation of aortic signal.Discussion and Conclusion
In this preliminary study, certain advantages and disadvantages for 2D and 3D QISS were evident. For instance, each 2D QISS image was acquired in only 1 RR interval (renal arteries) or 2 RR intervals (coronary arteries), thereby reducing sensitivity to respiratory motion and arrhythmias compared with the multiple cardiac cycles required for 3D QISS. Image quality for 2D QISS was not affected by the number of acquired slices, whereas 3D QISS image quality improved as the number of slices was increased due to signal averaging and reduced Gibbs ringing along the slice direction. Conversely, 3D QISS enhanced the depiction of small branch vessels, while the more rectangular slice profile improved image quality for multi-planar reconstructions. Other image quality differences related to the mechanisms for fat suppression used with the respective techniques. For instance, 2D QISS used a spatially non-selective chemical shift-selective RF pulse to suppress fat signal. This method for fat suppression was prone to inadvertent saturation of arterial signal in regions away from the magnet isocenter, such as the descending thoracic aorta when the acquisition was centered on the renal arteries. Consequently, it could not be reliably used for 2D QISS of the renal arteries. On the other hand, 3D QISS relied on intrinsic fat suppression from the FISS readout, which was restricted to the excited 3D slab. This method did not cause inadvertent arterial saturation or other artifacts for 3D QISS of the renal arteries.
In conclusion, 2D and 3D QISS appear to have complementary value for breath-hold MRA of the coronary and renal arteries. For instance, with 2D QISS, there is less concern about inadvertent saturation of arterial inflow as well as artifacts from respiratory motion and arrhythmias. With 3D QISS, one can acquire thinner slices, improve the depiction of small arterial branches and reduce blurring due to slice profile effects for multi-planar reconstructions.
Acknowledgements
NIH grants R01 HL130093 and R21 HL126015References
1. Edelman RR, Giri S, Pursnani A, Botelho MPF, Li W, Koktzoglou I. Breath-hold Imaging of the Coronary Arteries using Quiescent-Interval Slice-Selective (QISS) Magnetic Resonance Angiography: Pilot Study at 1.5 Tesla and 3 Tesla. J Cardiovasc Magn Reson 2015 Nov; 17:101. PMID 26597281 PMCID.
2. Edelman RR, Silvers RI, Thakrar KH, Metzl MD, Nazari J, Giri S, Koktzoglou I. Nonenhanced MR angiography of the pulmonary arteries using single-shot radial quiescent-interval slice-selective (QISS): a technical feasibility study. J Cardiovasc Magn Reson. 2017 Jun 30;19(1):48. doi: 10.1186/s12968-017-0365-3.
3. Koktzoglou I, Edelman RR. Radial fast interrupted steady-state (FISS) magnetic resonance imaging. Magn Reson Med. 2017 Aug 30. doi: 10.1002/mrm.26881. [Epub ahead of print]
Figures