2987
Large Field-of-View Nonenhanced Neurovascular MR Angiography Using Ungated Radial Quiescent-Interval Slice-Selective (QISS)1Radiology, NorthShore University HealthSystem, Evanston, IL, United States, 2Radiology, University of Chicago Pritzker School of Medicine, Chicago, IL, United States, 3Radiology, Northwestern University Feinberg School of Medicine, Chicago, IL, United States, 4Siemens Healthineers, Chicago, IL, United States
Synopsis
We report a prototype ungated radial quiescent-interval slice-selective technique for nonenhanced magnetic resonance angiography of the extracranial carotid, vertebrobasilar and proximal intracranial circulations. The proposed method efficiently covers a large field-of-view, provides improved image quality with respect to Cartesian sampling, and provides flexibility to shorten the acquisition time via radial undersampling.
Introduction
Recent work
has shown that quiescent-interval slice-selective (QISS) can be used for nonenhanced
magnetic resonance angiography (MRA) of the extracranial and intracranial circulations
with the potential for improved image quality and background suppression with
respect to non-enhanced time-of-flight MRA.1,2 To date, QISS protocols have mainly used cardiac
gating as well as Cartesian k-space sampling trajectories. In this work, we hypothesized that QISS using
radial k-space sampling might provide large coverage for neurovascular MRA
spanning both the extracranial and intracranial circulations, without the need
for cardiac gating. Our aims were to:
(1) test an ungated radial implementation of QISS for extracranial and
intracranial MRA; (2) compare the approach with Cartesian k-space sampling; and
(3) evaluate the impacts of slice orientation and radial undersampling on image
quality.Methods
Imaging was performed on 4 healthy volunteers at 3 Tesla (MAGNETOM Skyra Fit, Siemens Healthcare, Erlangen, Germany) under an IRB-approved protocol. A prototype QISS MRA protocol was implemented with a radial fast low-angle shot (FLASH) readout. Static tissue and veins were suppressed with the application of in-plane and tracking adiabatic inversion pulses.
Baseline QISS imaging parameters were as follows: 96 2.0 mm-thick slices acquired with 0.66 mm overlap, slice acquisition tilt of 60 degrees with respect to the axial plane, 416 mm field-of-view, 1.0/0.5mm acquired/reconstructed spatial resolution, TR/TE/flip of 15 msec/4.9 msec/30 degrees, 501 Hz/pixel receiver bandwidth, 3 shots (i.e. QISS repetitions) per slice, 204 views / lines acquired for radial / Cartesian sampling (i.e. 68 per shot), shot repetition time of 1068 msec and 530 msec inflow time (from time of inversion to echo train center). Radial sampling used golden angular view increments. Scan times for 3-shot, 2-shot (radial only), and single-shot (radial only) QISS protocols were 5 min 7 sec, 3 min 25 sec, and 1 min 42 sec, respectively.
The impact of k-space trajectory was assessed by comparing 3-shot radial and 3-shot Cartesian protocols. The influence of slice orientation was evaluated by comparing 3-shot radial protocols acquired with slice tilts of 45, 60, and 67.5 degrees away from the axial plane. The impact of radial undersampling was probed by comparing images obtained with single-shot, 2-shot, and 3-shot radial protocols.
Quantitative estimates of arterial signal-to-noise ratio (SNR), arterial-to-muscle contrast-to-noise ratio (CNR), and arterial-to-muscle contrast were made at the level of the distal common carotid artery. Qualitative analysis consisted of a radiologist scoring 18 arterial segments for image quality using a 4-point scale (1: non-diagnostic, 2: fair, 3: good, 4: excellent). The proportion of arterial segments rated as “good” or “excellent” was tabulated.
Results
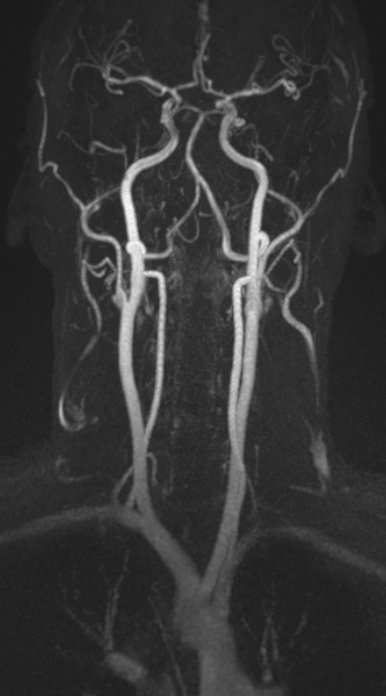
Ungated QISS MRA using radial sampling and a FLASH readout covered the extracranial carotid, vertebral and proximal intracranial arteries in approximately 5 minutes for a 3-shot protocol (Figure 1) and under 2 minutes for a single-shot protocol. Radial sampling provided comparable to better SNR, CNR and imaging contrast than Cartesian sampling. For 3-shot protocols, radial sampling was slightly preferred to Cartesian sampling in terms of image quality (3.7 vs. 3.6; P<0.05). The proportion of segments rated with good or excellent image quality differed between the three slice acquisition tilts (P<0.001): 96%, 79%, and 79% for 3-shot QISS protocols using 60 degree, 45 degree, and 67.5 degree tilts, respectively. Proximal and distal arterial segments were better displayed with slice tilts >45 degrees (P<0.01), possibly due to greater spatial coverage. Image quality for radial QISS improved as the number of shots was increased from 1 to 3 (3.1 [single-shot] vs. 3.3 [2-shot] vs. 3.7 [3 shot]; P<0.001). The proportion of segments rated with good or excellent image quality was 96% for 3-shot imaging, 86% for 2-shot imaging, and 72% for single-shot imaging (P<0.001).Discussion
Ungated QISS MRA using radial sampling and a FLASH readout can display the full lengths of the extracranial carotid and vertebral arteries, as well as the proximal intracranial arteries in approximately 5 minutes for 3-shot imaging, and in under 2 minutes for single-shot imaging. Radial sampling was slightly preferred over Cartesian sampling in terms of image quality, 60 degree slice tilts (with respect to the axial plane) were favored over 45 and 67.5 degree tilts, and image quality was optimized with the use of a 3-shot protocol.Conclusion
Radial ungated QISS FLASH MRA is a promising approach for efficient and high quality evaluation of the extracranial and proximal intracranial circulations within a single acquisition. Given the improvement in image quality and higher scan efficiency, with further validation it has the potential to supplant existing time-of-flight approaches for evaluation of the extracranial carotid, vertebrobasilar, and proximal intracranial circulations.Acknowledgements
NIH grants R01 HL130093 and R21 HL126015.References
1. Koktzoglou I, Murphy IG, Giri S, Edelman RR. Quiescent interval low angle shot magnetic resonance angiography of the extracranial carotid arteries. Magn Reson Med. 2016 May;75(5):2072-7. doi: 10.1002/mrm.25791.
2. Koktzoglou I, Edelman RR. Super-resolution intracranial quiescent interval slice-selective magnetic resonance angiography. Magn Reson Med. 2017 May 3. doi: 10.1002/mrm.26715.
Figures