2984
Whole-heart coronary MRA at 3.0T: Comparison between conventional method and new acceleration technique by compressed SENSE.1Department of Radiology, Mie University Hospital, Tsu, Mie, Japan, 2MR Clinical Science, Philips Japan, Ltd., Tokyo, Japan
Synopsis
Compressed SENSE (CSENSE) is a novel method to combine Sensitivity Encoding (SENSE) and compressed sensing for rapid MR imaging. CSENSE can achieve a reduction factor higher than those achieved by SENSE while preserving the image quality by the denoising effect with iterations. In this work, CSENSE was applied to 3.0T free-breathing whole-heart coronary MRA to reduce the acquisition time. As compared to the conventional acquisition method using SENSE, CSENSE allows for up to 2.5-fold reduction of acquisition time without significant degradation of image quality of whole-heart coronary MRA at 3.0T, especially after the contrast injection.
Introduction
Free-breathing whole-heart coronary MR angiography (MRA) is an established method that can clearly visualize coronary arteries with a narrow acquisition window in the cardiac cycle. However, a long acquisition time is a major limitation of whole-heart coronary MRA (1). Parallel imaging (PI) is a well-established method for scan acceleration in MRI, while compressed sensing (CS) is an emerging technique to accelerate conventional MRI by reducing the number of acquired data based on CS theory. The combination of PI and CS is of great interest to further accelerate MRI scans (2-4). Recently, a novel method to combine sensitivity encoding (SENSE), one of the standard methods for PI, and CS for rapid MR imaging has been proposed and named compressed SENSE (CSENSE). CSENSE can achieve a reduction factor higher than those achieved by SENSE while preserving the image quality by the denoising effect with iterations. In this work, CSENSE was applied to 3.0T free-breathing whole-heart coronary MRA to reduce the acquisition time. The purpose of this study was to evaluate if CSENSE can reduce the acquisition time of 3.0 T whole-heart coronary MRA without degradation of image quality compared to a conventional whole-heart coronary MRA using SENSE.Methods
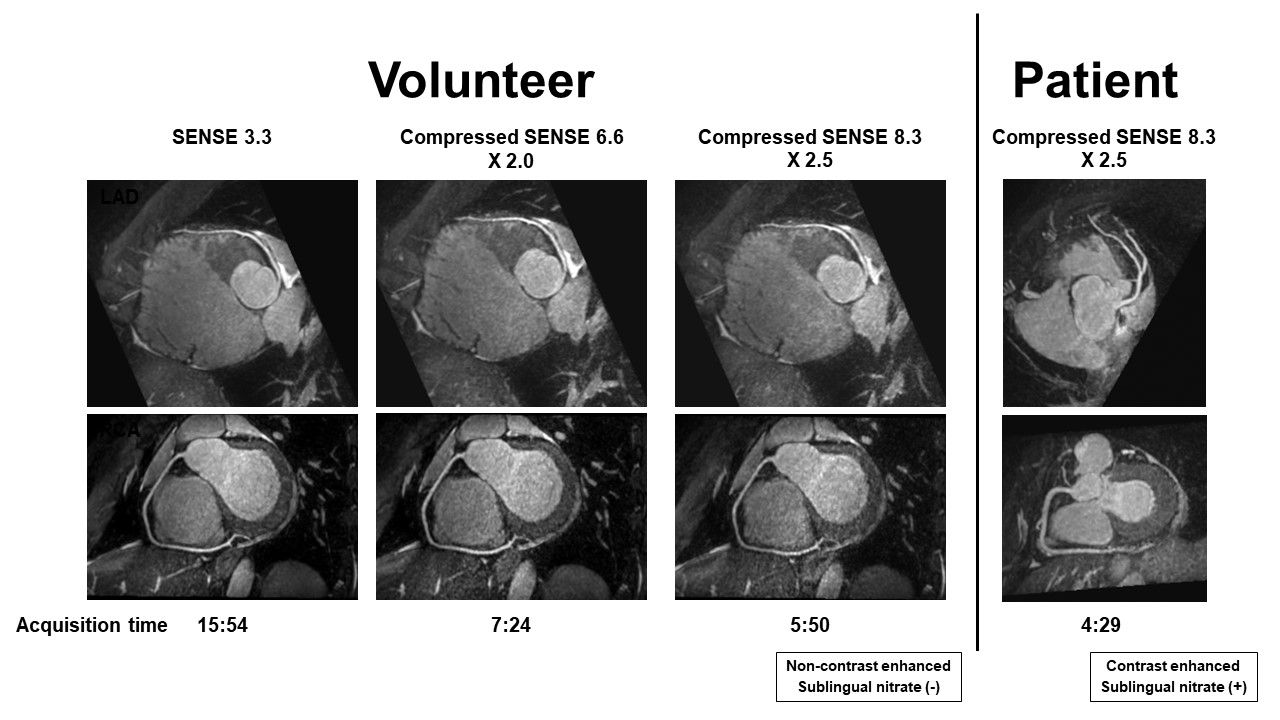
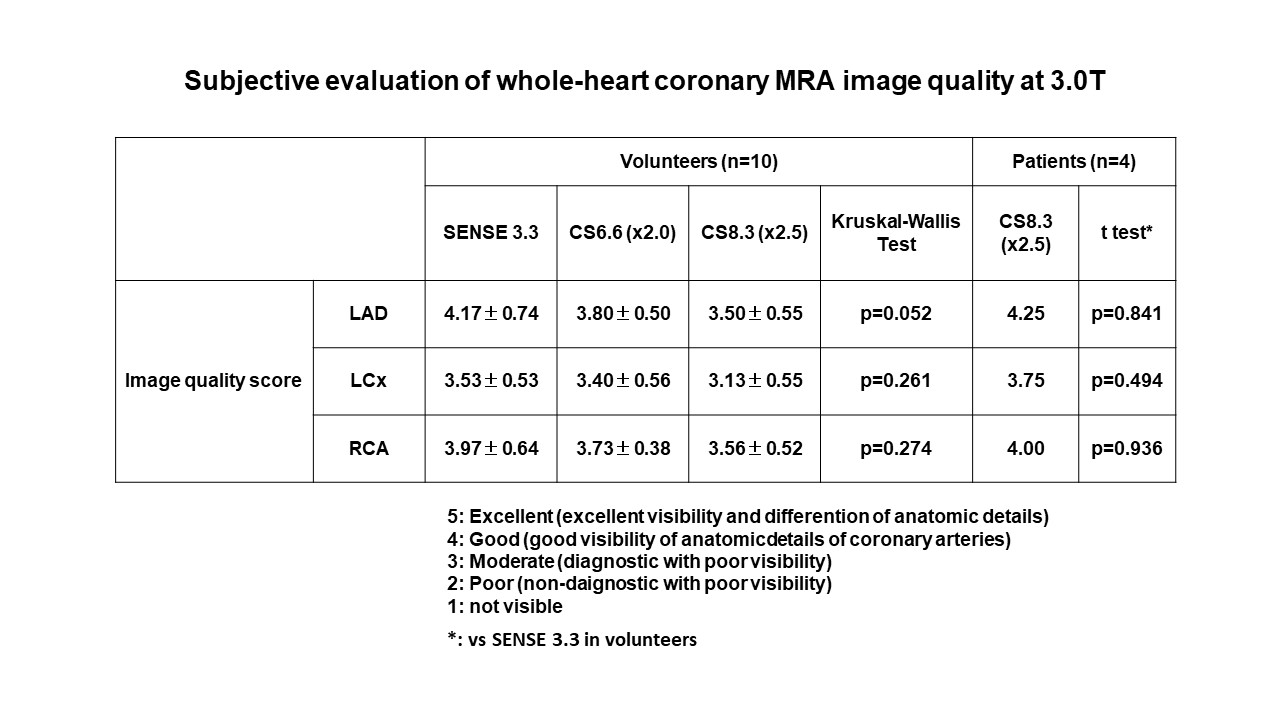
Ten healthy volunteers (31±9 years, 10 male) were scanned (Ingenia 3.0T, Torso coil, Philips Healthcare, Best, Netherlands). After preparatory scans for localization of the heart, B1 calibration and identification of the coronary resting period, 3D transverse whole-heart coronary MRA images were acquired during free breath using a fast segmented gradient echo (TFE) sequence with T2 preparation and fat saturation (TR/TE/flip angle=3.6/1.65/15; full Fourier encoding; acquisition duration per cardiac cycle = 50ms; navigator gating window = 4mm; resolution =0.64x0.64x0.8mm; k-space encoding = radial; slab thickness = adapted). The following 3 settings were compared: SENSE=3.3, CSENSE=6.6, CSENSE=8.3 (conventional setting, 2-, and 2.5-fold acceleration of conventional setting, respectively). The acquisition order was randomized in each subject. Then, 4 patients with suspected coronary artery disease (CAD) underwent whole-heart coronary MRA after late gadolinium enhanced (LGE) MRI with the standard administration of gadolinium contrast medium using the same imaging parameter with CSENSE=8.3. Acquisition time was recorded. Vessel sharpness and diameter were determined for the proximal portion of right and left coronary arteries. Signal to noise ratio (SNR) was determined in LV myocardium and blood in LV outflow tract. Contrast to noise ratio (CNR) were determined in blood in LV outflow tract. Three blinded observers assessed a subjective image quality for the right and left coronary arteries using 5-pint scale (5: excellent, 4: good, 3: moderate, 2: poor, 1: not visible).Results
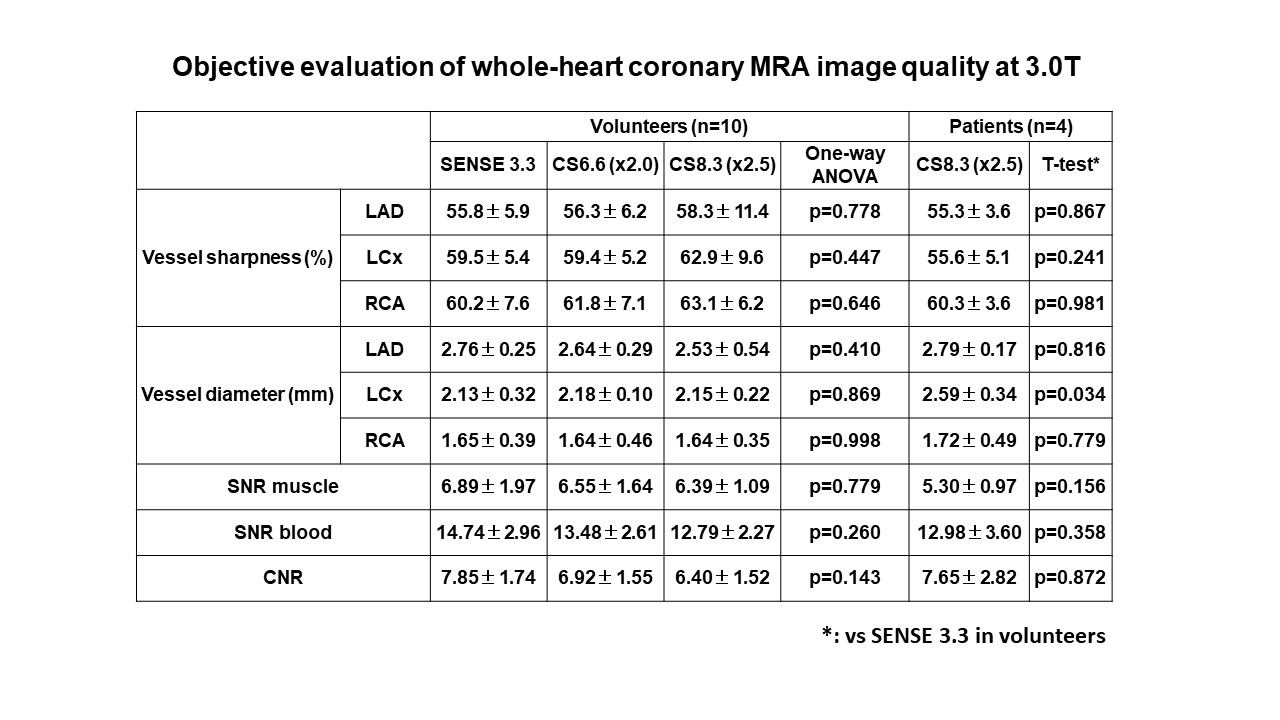
In 10 volunteers, acquisition time for CSENSE=8.3 (6.1min±111s) and that for CSENSE=6.6 (7.4min±94s) was 43% and 51% of that for conventional setting (SENSE=3.3) (14.3min±119s), respectively. In 4 patients, acquisition time was 2.8min±59s (CSENSE=8.3). Representative images were shown in Figure 1. In the volunteers, no significant difference was observed in the vessel sharpness and diameter in LAD (p=0.778, p=0.410), LCx (p=0.447, p=0.869) and RCA (p=0.646, p=0.998) among the 3 settings, respectively (Table 1). Myocardial SNR (6.89±1.97, 6.55±1.64, 6.39±1.09, p=0.779), blood SNR (14.74±2.96, 13.48±2.61, 12.79±2.27, p=0.260) and CNR (7.85±1.74, 6.92±1.55, 6.40±1.52, p=0.143) showed no significant difference among the 3 settings (SENSE=3.3, CSENSE=6.6, CSENSE=8.3, respectively) with the trend of reduction in each value with increasing acceleration factors. Blood CNR of whole-heart coronary MRA with CSENSE=8.3 after LGE MRI in the patients (7.65±2.82) was substantially greater than that of non-contrast whole-heart coronary MRA with CSENSE=8.3 in healthy volunteers (6.40±1.52, p=0.29) and comparable to that with conventional setting in healthy volunteers (7.85±1.74, p=0.87). Image quality score was not significantly different among 3 settings in LAD (p=0.052), LCx (p=0.261) and RCA (p=0.274) in the volunteers having the trend of reduction with increasing acceleration factors (Table 2). Subjective image quality score of 2.5-fold accelerated coronary MRA as compared to conventional setting after LGE MRI in patients were comparable to that of non-contrast coronary MRA with conventional setting in healthy volunteers (Table 2).Discussion and conclusion
Scan acceleration by CSENSE allows for significant reduction of total acquisition time of whole-heart coronary MRA at 3.0T. Up to 2.5-fold acceleration by CSENSE as compared to the conventional acquisition using SENSE, image quality of non-contrast whole-heart coronary MRA is maintained despite of the slight reduction of SNR and CNR. The administration of contrast medium may compensate for the reduced SNR and CNR of whole-heart coronary MRA accelerated by CSENSE. 3.0T whole-heart coronary MRA accelerated by CSENSE allows for noninvasive imaging of the coronary arteries with adequate image quality and substantially reduced scan time.Acknowledgements
No acknowledgement found.References
1. Kato S, et al. J Am Coll Cardiol. 2010; 56:983-991.
2. Doneva M, et al. Proc. of ISMRM 2012; #20
3. Liang D, et al. Magnetic Resonance in Medicine. 2009; 62:1574-1584.
4. Uecker M, et al. Magnetic Resonance in Medicine. 2014; 71:990-1001.
Figures