2970
Comparison of cardiac MRI myocardial strain quantification techniques demonstrates systematic differences between feature tracking and heart deformation analysis1Department of Radiology, Northwestern University, Chicago, IL, United States, 2Medicine - Cardiology, Northwestern University, Chicago, IL, United States, 3Biomedical Engineering, Northwestern University, Evanston, IL, United States
Synopsis
Introduction:
Cardiac myocardial strain is useful for detecting early manifestations of cardiac dysfunction and may predict adverse outcomes. (1) Speckle tracking echocardiography (STE) is considered a reference standard for myocardial strain (2, 3); however, STE has known limitations with inherently low contrast resolution and narrow acoustic windows. Cardiac MR (CMR) is the reference standard for biventricular systolic function, and enable tissue characterization in a single examination. Myocardial strain is increasingly being peformed at cardiac MRI in multiple clinical settings. Multiple different CMR strain techniques are available which differ in the tissue tracking algorithm and strain calculation. Although dedicated displacement and strain encoding techniques are available, these have suffered from limited adoption due to the need for dedicated post-processing software and dedicated acquisitions. Several strain methods are available which enable retrospective analysis of balanced steady state free precession (bSSFP) cine imaging for myocardial strain analysis. Heart deformation analysis (HDA) relies on an inverse consistent deformable registration algorithm to general myocardial strain data. (4) Feature tracking (CMR-FT) relies on tracking different imaging features throughout time; the specific features are depending on the specific algorithm. The purpose of this study is to compare CMR derived myocardial strain values in a cohort of HIV positive patients using HDA and CMR-FT.Methods:
A total of 30 HIV positive patients (age = 50.2 ± 11.7 25 men, 5 women), out of which 22 patients have adjudicated heart failure, were obtained from an electronic database of HIV patients maintained at our institution. In this retrospective study, all MRI exams were performed using 1.5 T MRI systems (Area, and Avanto; Siemens, Germany). bSSFP cinegraphic MRI was performed in short axis (SA) at the base, mid, and apex and in the 4 chamber (4Ch) and 2 chamber (2Ch) long axis orientations. Images were acquired during suspended respiration with retrospective ECG gating (spatial resolution: 1.4-2.0 x 1.4-2.0 x 6-8 mm3, TR: 32-68 ms, TE: 1.1-1.5 ms, flip angle: 54-80o).
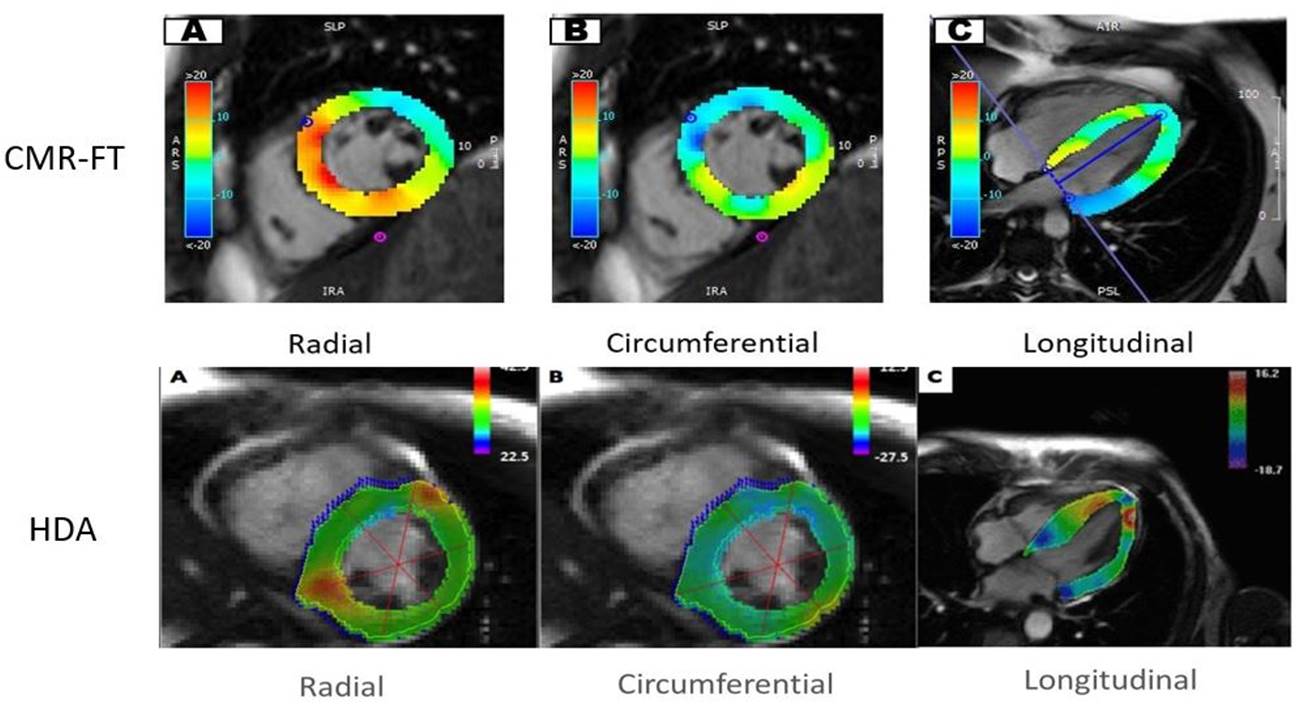
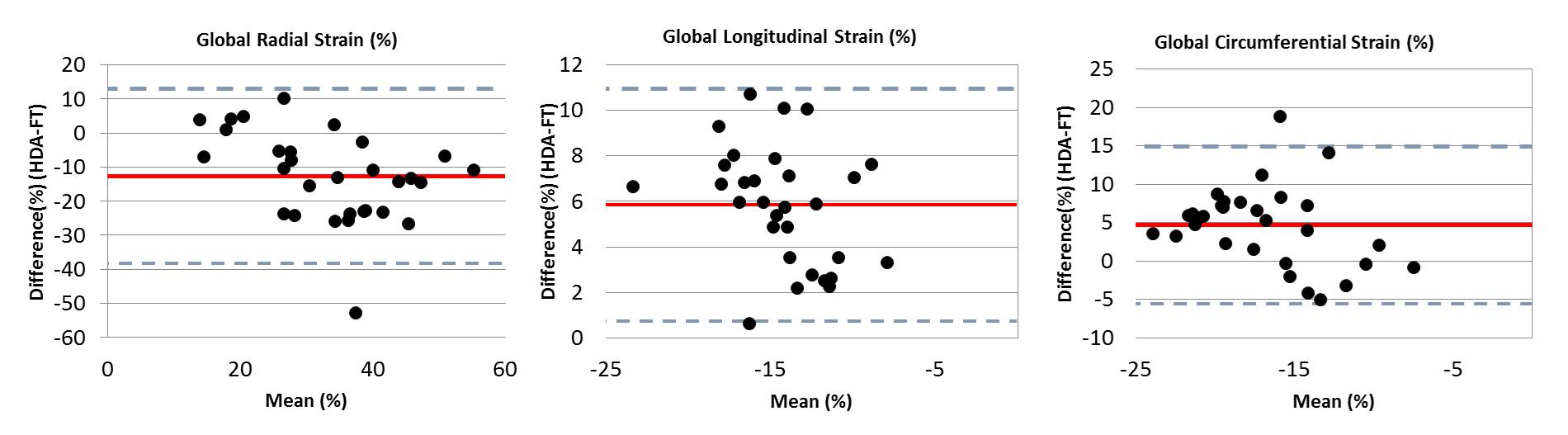
MR cardiac strain analysis was performed using dedicated software for each technique (HDA: Trufi Strain, [prototype software] Siemens, Princeton, NJ, USA; CMR-FT: cvi42, Circle Cardiovascular Imaging, Inc. Calgary, Canada). The HDA and CMR-FT were used to retrospectively quantify the global and regional (base, mid, apex) radial (Err) and circumferential (Ecc) Lagrangian strain, and global longitudinal Lagrangian (GLS) myocardial strain values using the bSSFP SA and long axis cine images (Figure 1). Global and regional Err and Ecc and GLS were compared between the two techniques using a paired t-test. The global Err, Ecc, and GLS were further evaluated using Bland Altman analysis (Figure 2) with results presented as mean difference [-1.96SD, +1.96SD].
Results:
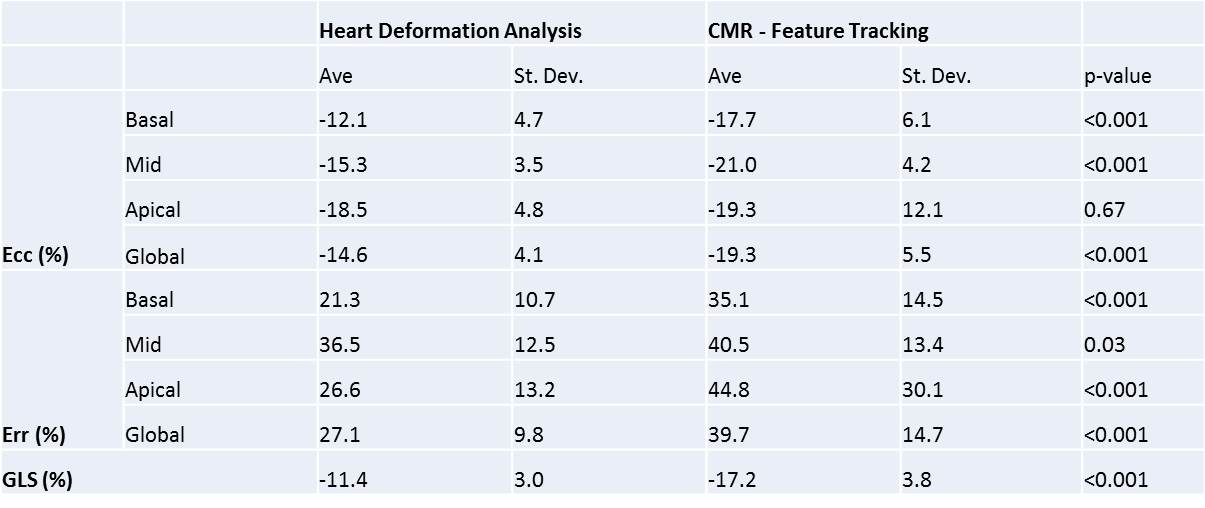
Strain was successfully calculated in all 30 patients using both HDA and CMR-FT. Global and regional Ecc and Err, and GLS were all significantly higher using CMR-FT relative to HDA, with the exception of the apical Ecc. Bland Altman analysis confirmed this observation demonstrating higher strain magnitudes by CMR-FT for Ecc (4.7% [-5.6%,14.9%]), Err (-12.6% [-38.2%,13.0%]), and GLS (5.8%[0.7%,10.9%]). To put these differences in context, CMR-FT yields higher strain values relative to HDA by 32% for global Ecc, 47% for Err, and 51% for GLS (Table 1). The myocardial strain standard deviation derived from HAD was reduced compared to CMR-FT for all comparisons.Conclusions:
Our results demonstrate significant differences in myocardial strain derived using HDA and CMR-FT in a HIV+ patient cohort with and without HF. Both HDA and CMR-FT are appealing CMR strain analysis methods as they calculate strain directly from bSSFP cine images enabling retrospective assessment of myocardial strain data. However, we demonstrated a systematic bias of CMR-FT for higher myocardial strains relative to HDA. It is also notable that HDA had relatively lower standard deviations for all strain calculations, suggesting that HDA may be a more consistent methods for measuring myocardial strain. There is a need for technique specific normative CMR strain values across to enable clinical applications of CMR derived myocardial strain data.Acknowledgements
No acknowledgement found.References
1. van Everdingen WM, Zweerink A, Nijveldt R, Salden OAE, Meine M, Maass AH, et al. Comparison of strain imaging techniques in CRT candidates: CMR tagging, CMR feature tracking and speckle tracking echocardiography. Int J Cardiovasc Imaging. 2017.
2. Lamacie MM, Thavendiranathan P, Hanneman K, Greiser A, Jolly MP, Ward R, et al. Quantification of global myocardial function by cine MRI deformable registration-based analysis: Comparison with MR feature tracking and speckle-tracking echocardiography. Eur Radiol. 2017;27(4):1404-15.
3. Keller EJ, Fang S, Lin K, Freed BH, Smith PM, Spottiswoode BS, et al. The consistency of myocardial strain derived from heart deformation analysis. Int J Cardiovasc Imaging. 2017;33(8):1169-77.
4. Ref: Guetter et al. Proc. ISBI, 2011
Figures