2963
Multiple sets of simultaneous multi-slice (SMS) for improved short and long axis coverage of myocardial DCE perfusion1Radiology and Imaging Sciences, University of Utah, Salt Lake City, UT, United States, 2Cardiology, University of Utah, Salt Lake City, UT, United States, 3Physics, University of Utah, Salt Lake City, UT, United States
Synopsis
We propose a unique perfusion acquisition that offers improved coverage and confidence of detecting true ischemia and artifacts in cardiac perfusion dynamic acquisitions. Three slices are acquired simultaneously after each saturation pulse, and there is time to acquire 3 sets of such slices even at high heartrates. The ability to simultaneously acquire multiple slices opens up many new possibilities. The approach proposed here can acquire for example 6 short axis slices and 3 long axis slices each heartbeat, which allows detection of small areas of ischemia and can provide additional volume coverage and confidence. Preliminary results show the promise of this multi-plane SMS approach.
Introduction
Dynamic contrast enhanced (DCE) MRI of the heart for detecting and characterizing coronary artery disease is becoming a more widespread tool. In such studies, stress and rest acquisitions are performed. The first pass of gadolinium contrast is tracked by imaging a number of slices sequentially each heartbeat. The number of slices is limited by the time in one heartbeat. Typically 2-4 short axis slices are acquired per beat, depending on heartrate. New simultaneous multi-slice (SMS) methods with controlled aliasing (CAIPI) allow for greater coverage. Such methods have been used with Cartesian1 and radial2-4 readouts. The additional noise or leakage from this approach is small when multi-band (MB) factors of 2-3 are used. Here we propose to acquire 3 sets or “blocks” of SMS slices, each with 3 simultaneous slices. Thus 9 slices are acquired per beat, at heartrates up to 120 beats per minute. The 9 slices can be acquired all short axis, or, it may be preferable to acquire one of the sets of slices as long axis slices, which could possibly increase the coverage or the confidence of ischemia that is found in intersecting regions that are common to the short and long axis views. Others have acquired a mixture of short and long axis slices previously, by reducing the number of short axis slices or by alternating the slice orientation between even and odd heartbeats (reduced temporal resolution). Including SMS allows new and beneficial trade-offs for myocardial perfusion coverage, which we formulate here.
Methods
A saturation recovery radial turboFLASH sequence was used in 4 subjects to study the potential of the multi-plane SMS cardiac perfusion imaging. TR/TE=2.7/1.6msec, FOV=260mm, ~1.8x1.8x8mm pixel size on a 3T Prisma (Siemens) scanner. Three slices were acquired simultaneously with the radial CAIPI SMS method5, 6. 30 rays (golden ratio ordering) were acquired after each saturation pulse, with a delay of ~80msec. With this delay the total acquisition time for 9 slices was < 500msec, so heartrates up to 120 could acquire the full 9 slices every beat. Scans were done at regadenoson stress, and ~20min. later at rest, both with ~0.75mmol/kg gadoteridol. Free-breathing scans were acquired. Image reconstruction: For each set of the simultaneously acquired slices, the 3 slices were reconstructed jointly with an iterative compressed sensing SMS method. The reconstruction included the sensitivity maps created from each coil by summing all of the time frames and using adaptive combine7. Temporal and spatial total variation constraints were included. In addition, in one subject single slices (SMS with multi-band (MB)=1) were acquired separately, ~10 minutes after contrast was administered. The SMS with MB=3 sequence was also repeated at that time, in order to compare the image quality directly.Results/Discussion
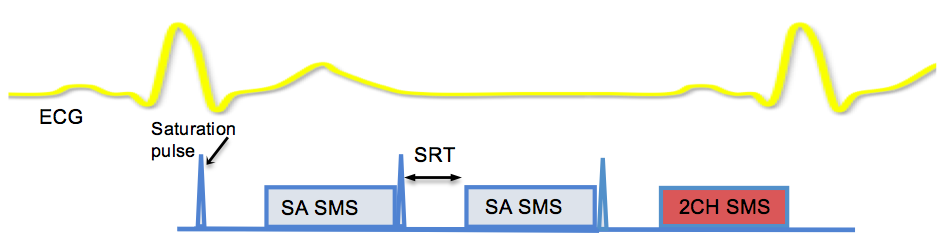
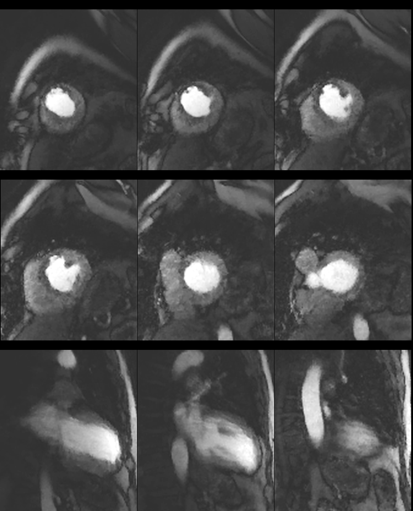
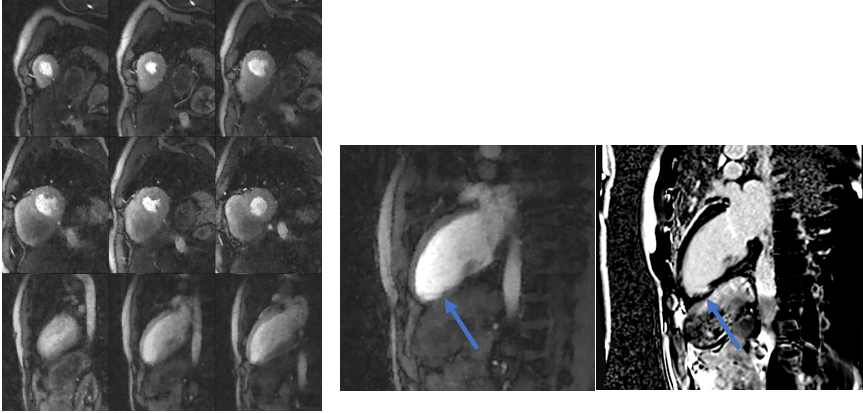
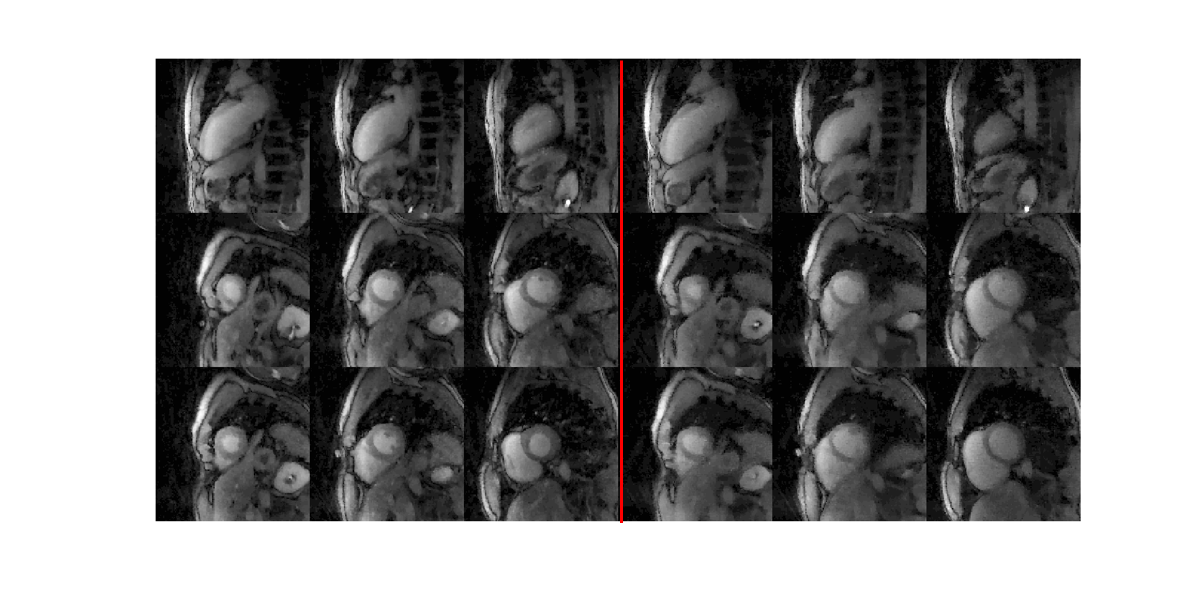
Fig. 1 shows the multi-planar SMS acquisition timings. In two subjects, 9 short axis slices were acquired rather than 6 short axis and 3 long axis slices. Two chamber long axis views were used since with free-breathing these slices typically have much less out-of-plane motion than four chamber slices. The perfusion acquisition is very similar to standard methods, but more slices are acquired, essentially for free. Fig. 2 shows an example from a subject that had X-ray angiography a year previous (total LAD occlusion, partial right coronary artery occlusion, bypasses of both vessels were done). Fig. 3, subject had distal occlusions of a diagonal and apical LAD. SMS with 3 slices is compared to single slice acquisitions in Fig. 4. SMS shows essentially no visible degradation. Four simultaneous slices is possible but would likely work better with breath-holding, and can be more dependent on coils and slice orientations. The temporal resolution of the SMS readouts is better than 3D acquisitions but as in 3D, the slices in each set are acquired simultaneously so have similar respiratory motion and cardiac cycle. The studies here show that the multi-plane SMS approach has promise for characterizing coronary artery disease and has unique advantages. More studies are needed to further evaluate the technique.Acknowledgements
This research was supported by the National Heart, Lung, And Blood Institute of the National Institutes of Health under Award Number R01HL138082. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.References
1. Stab D, Wech T, Breuer FA, Weng AM, Ritter CO, Hahn D, Kostler H. High resolution myocardial first-pass perfusion imaging with extended anatomic coverage. J Magn Reson Imaging. 2014;39:1575-1587
2. Adluru G, Chen L, DiBella EVR. Radial CAIPI-CS for simultaneous multi-slice cardiac perfusion imaging. Proc Int Soc Magn Reson. 2014:1532
3. Wang H, Adluru G, Chen L, Kholmovski EG, Bangerter NK, DiBella EV. Radial simultaneous multi-slice CAIPI for ungated myocardial perfusion. Magn Reson Imaging. 2016;34:1329-1336
4. Rosenzweig S, Holme HCM, Wilke RN, Voit D, Frahm J, Uecker M. Simultaneous multi-slice MRI using cartesian and radial FLASH and regularized nonlinear inversion: SMS-NLINV. Magn Reson Med. 2017
5. Tian Y, Adluru G, Mendes J, DiBella E. Optimized 2D radial CAIPIRINHA for cardiac perfusion MRI. ISMRM. 2017;44
6. Chen W, Gillett E, Khoo MCK, Davidson Ward SL, Nayak KS. Real-time multislice MRI during continuous positive airway pressure reveals upper airway response to pressure change. J Magn Reson Imaging. 2017;46:1400-1408
7. Walsh DO, Gmitro AF, Marcellin MW. Adaptive reconstruction of phased array MR imagery. Magn Reson Med. 2000;43:682-690
Figures