2961
Simultaneous Multi Slice (SMS) SSFP first-pass myocardial perfusion imaging with iterative reconstruction at 1.5 Tesla.1Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 2MR Research Collaborations, Siemens Healthcare Limited, Frimley, United Kingdom, 3Siemens Healthcare, Erlangen, Germany, 4The Centre for Advanced Imaging, The University of Queensland, Brisbane, Australia
Synopsis
Myocardial perfusion imaging is recommended for ischaemia testing in patients although spatial coverage is limited to 3 slices in clinical practice. Simultaneous Multi Slice (SMS) imaging combined with iterative reconstruction was evaluated to provide greater heart coverage with minimal signal-to-noise penalty. 8 patients underwent two contrast enhanced dynamic perfusion scans at rest to compare the standard 3 slice with the SMS 6 slice protocol. Subjective image quality was found to be comparable to a standard 3 slice approach. This technique may have clinical utility in patients with suspected coronary artery disease through detection of ischaemia with greater heart coverage.
Introduction
In routine clinical practice, conventional first-pass contrast-enhanced cardiovascular magnetic resonance (CMR) perfusion imaging has limited spatial coverage, usually 3 slices. There are emerging techniques for greater spatial coverage which may provide improved confidence in clinical reporting and may allow for detection of perfusion defects that may not be detected in a standard 3 slice approach. Simultaneous multi-slice (SMS) imaging is an acceleration technique which enables simultaneous acquisition of multiple slices to increase spatial coverage of CMR perfusion 1 with minimal signal-to-noise (SNR) penalty. Robustness of SMS-bSSFP against B0 inhomogeneities can be ensured by adding Gradient Controlled Local Larmor Adjustment (GC-LOLA). 2 The signal to noise penalty of the accelerated SMS acquisition can be mitigated using iterative reconstruction for denoising. 3 In this study, we sought to evaluate CMR rest perfusion using an accelerated SMS GC-LOLA bSSFP prototype sequence combined with iterative reconstruction.Methods
Eight patients listed for a clinically indicated non-perfusion CMR scan were recruited and imaged at 1.5T (MAGNETOM Aera, Siemens Healthcare, Erlangen, Germany). Following patient consent, two rest contrast perfusion protocols using standard bSSFP imaging (3 slices) and SMS GC-LOLA bSSFP imaging (6 slices) were acquired in a random order in each patient using a dual-bolus technique 0.0075 + 0.075mmol/kg of Gadovist (Bayer, Berlin, Germany) as previously described. The two acquisitions were separated by a minimum time interval of 15 minutes to allow for contrast washout and the imaging parameters were matched between both sequences (TR/TE/α: 2.9ms/1.24ms/50° [SMS], TR/TE/α: 2.5ms/1.04ms/50° [standard], voxel size: 1.9x1.9mm2, slice thickness: 10mm, FOV: 332x332mm2, TI 120ms [SMS] 105ms [standard], bandwidth 1093Hz/px, TGRAPPA acquisition scheme, TGRAPPA factor: 2.5). SMS data were reconstructed using a non-linear iterative reconstruction with L1 regularization in wavelet space (referred to as SMS-iter). 3,5,6 Regularisation was performed both in space and time. 7 For comparison, standard bSSFP and SMS data were also reconstructed using standard TGRAPPA reconstruction. 8 Subjective assessment of image quality (4 = excellent, 3 = minor artefact and diagnostic image quality, 2= major artefact and diagnostic quality and 1= poor image quality and non-diagnostic) and circumferential percentage of dark rim artefact were assessed by consensus by two CMR experts blinded to the clinical details.Results
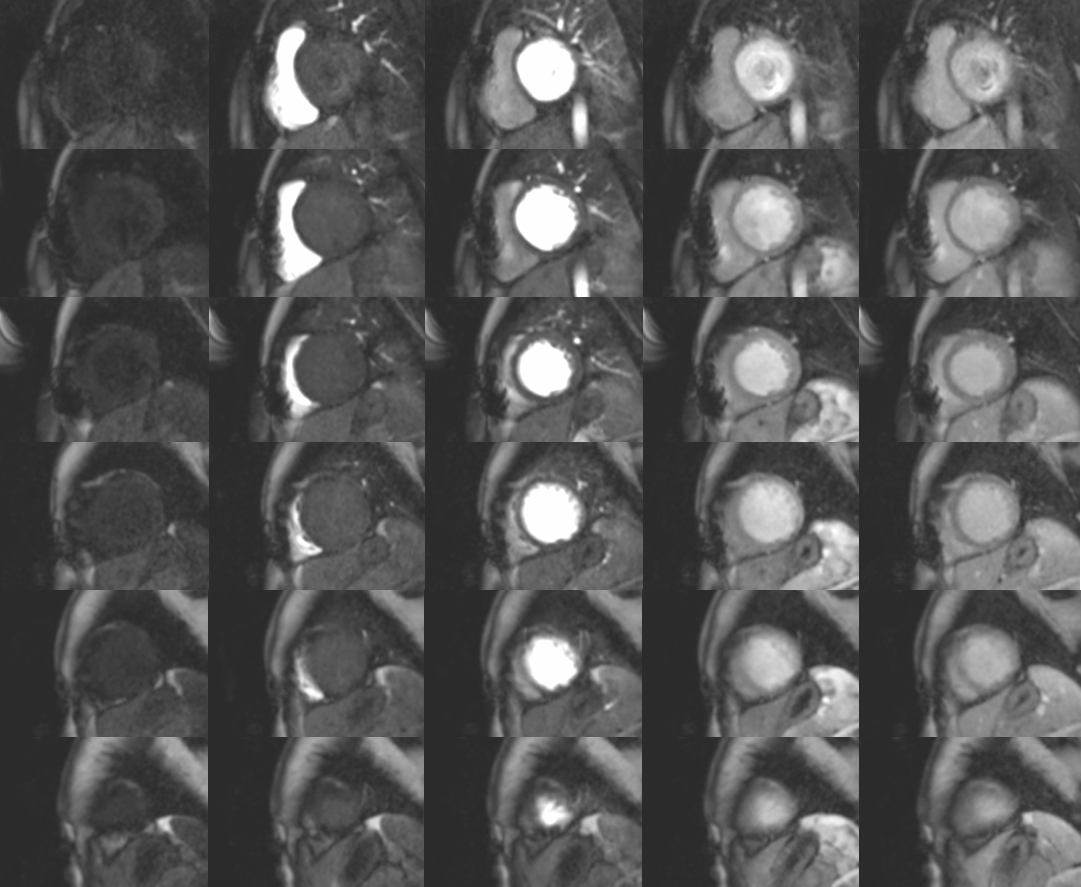
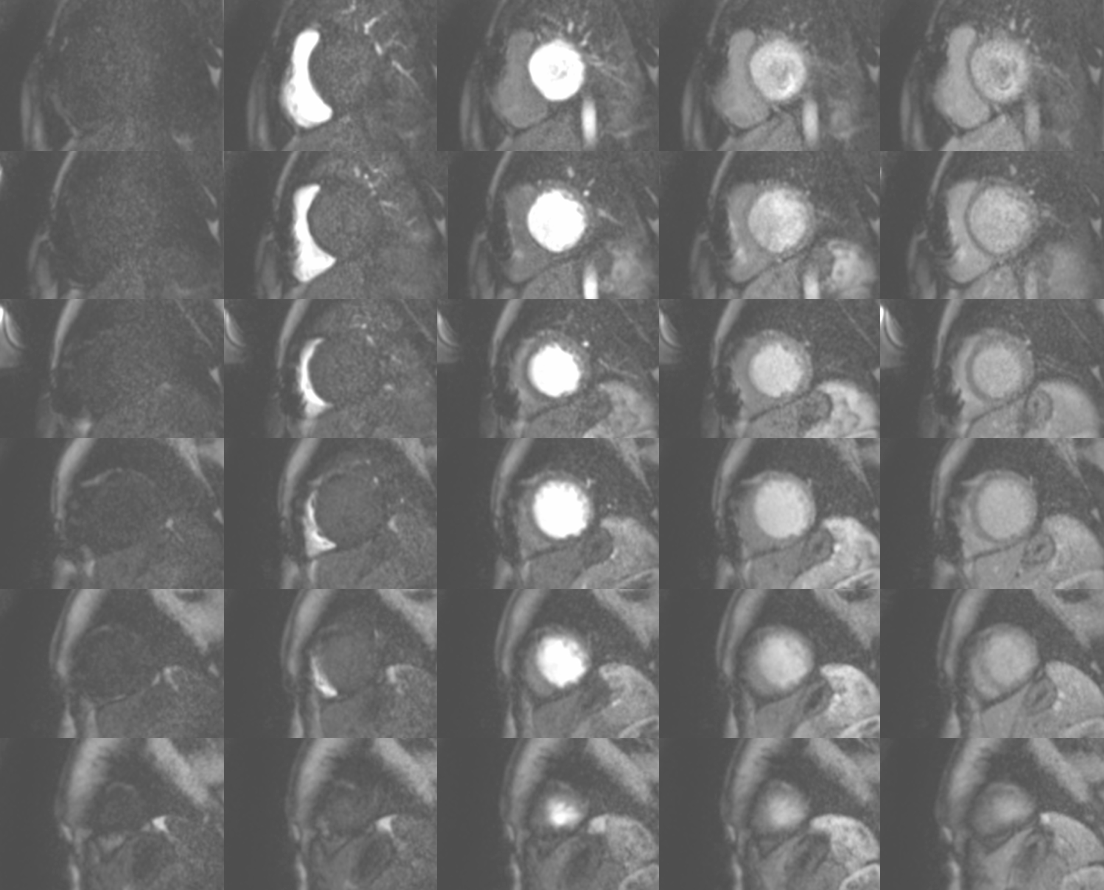
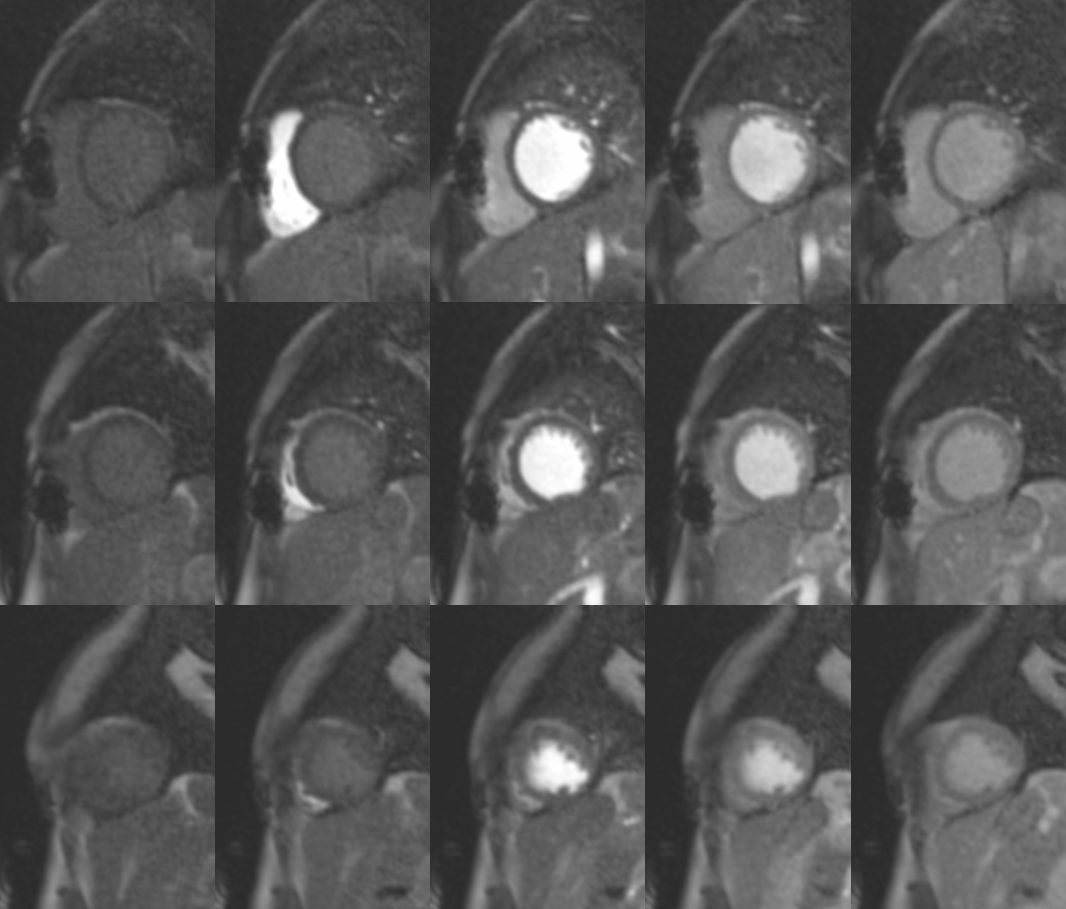
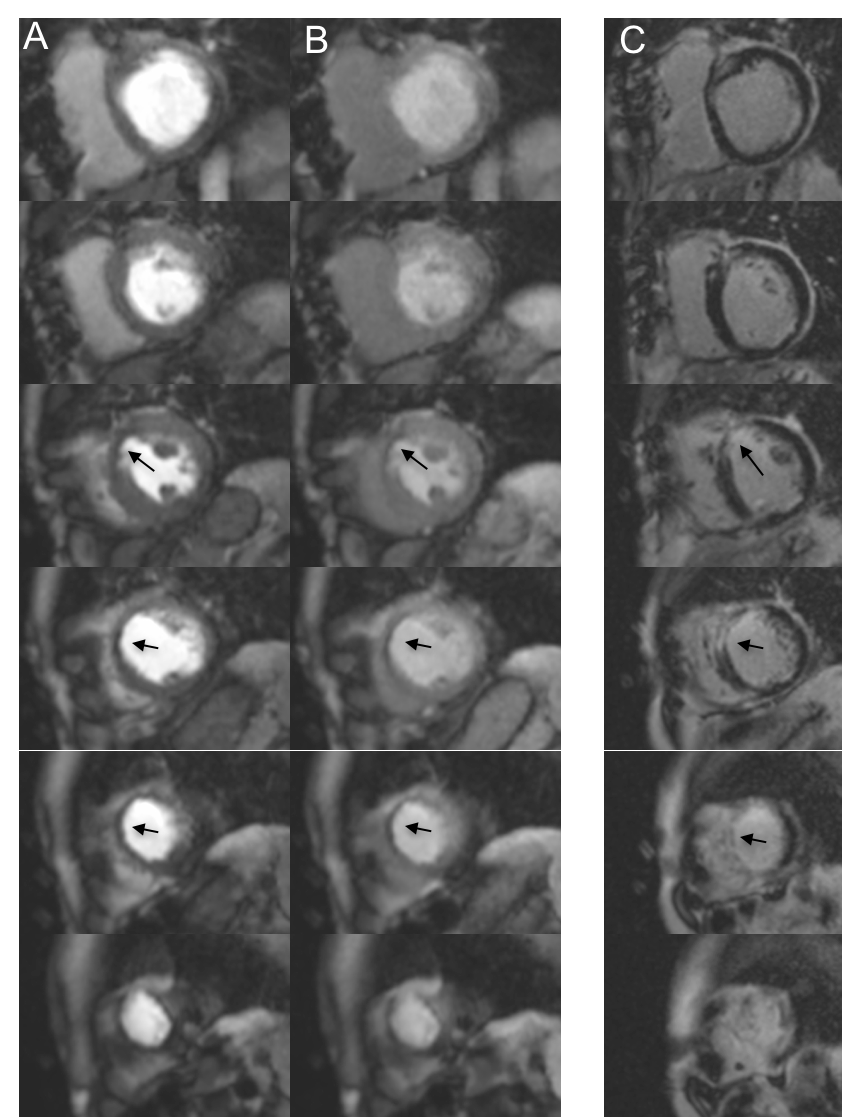
Images obtained using the SMS-TGRAPPA, SMS-iter and standard acquisition are shown in Figure 1, 2 and 3. Image quality scores obtained using standard 3-slice approach (2.2±0.9) and SMS-iter (2.1±0.8) were higher than SMS-TGRAPPA (1.6±0.9), although these were not statistically significant (p=0.33, Kruskal-Wallis test). There was no difference in degree of dark rim artefact between 3-slice, SMS-TGRAPPA and SMS-iter (12±23% vs. 4±4% vs. 7±8%, p =0.6, Kruskal-Wallis test). Figure 4 demonstrates the potential of SMS-iter for detection of perfusion defects in a patient with ischemic heart disease.Discussion
Lower image quality ratings were recorded in all sequences and this may be explained as the images were acquired during rest conditions, with low blood flow, relatively low peak contrast concentration in the myocardium and therefore low signal to noise ratio compared to stress protocols. Greater spatial coverage, as achieved using the proposed approach, is a desired feature for myocardial perfusion imaging. This technique may be clinically relevant as it may improve the sensitivity of detection of ischaemia through greater spatial coverage that may not otherwise be detected in a standard 3 slice approach. However, for true whole-heart perfusion imaging, more slices would be required than the 6 slices presented in this study. Finally, higher regularisation in the iterative reconstruction could provide further noise reduction but would also increase sensitivity to motion potentially arising in patients with poor breath holding ability. Further validation in a larger patient cohort with the addition of stress testing for maximal hyperaemia is thus required.Conclusions
We demonstrated the feasibility of myocardial perfusion imaging with greater spatial coverage using the SMS GC-LOLA technique. The addition of iterative reconstruction enhanced SMS GC-LOLA bSSFP image quality compared to TGRAPPA reconstruction and led to comparable image quality and artefact level as the standard 3 slice approach. Future evaluation in ischemic patients with myocardial scar and / or stress-induced perfusion defects will determine the clinical utility of this technique.Acknowledgements
This study received funding from NIHR Healthcare Technology Co-operative for Cardiovascular Disease at Guy’s and St Thomas’ NHS Foundation Trust and was supported by a fellowship from the Medical Research Council for MSN. This work was also supported by the Wellcome EPSRC Centre for Medical Engineering at King’s College London (WT 203148/Z/16/Z), and the EPSRC grant (EP/R010935/1).References
1. Stäb D, Wech T, Breuer FA et al. High resolution myocardial first-pass perfusion imaging with extended anatomic coverage. Journal of Magnetic Resonance Imaging 2014;39:1575-1587.
2. Speier P, Staeb D, Mueller E. CAIPIRINHA-accelerated 2D bSSFP imaging with improved banding behavior using Gradient-Controlled Local Larmor Frequency (GC-LOLA). Journal of Cardiovascular Magnetic Resonance 2016;18:P301.
3. Lustig M, Donoho D, Pauly JM. Sparse MRI: The application of compressed sensing for rapid MR imaging. MagnResonMed 2007;58:1182-1195.
4. Ishida M, Schuster A, Morton G et al. Development of a universal dual-bolus injection scheme for the quantitative assessment of myocardial perfusion cardiovascular magnetic resonance. JCardiovascMagnReson 2011;13:28.
5. Liang D, Liu B, Wang J, Ying L. Accelerating SENSE using compressed sensing. MagnResonMed 2009;62:1574-1584
6. Beck A, Teboulle M. A Fast Iterative Shrinkage-Thresholding Algorithm for Linear Inverse Problems. SIAM Journal on Imaging Sciences 2009;2:183-202.
7. Liu J, Lefebvre A, Zenge MO, Schmidt M, Mueller E, Nadar MS. 2D bSSFP real-time cardiac CINE-MRI: compressed sensing featuring weighted redundant Haar Wavelet regularization in space and time. Journal of Cardiovascular Magnetic Resonance 2013;15:P49-P49.
8. Breuer FA, Kellman P, Griswold MA, Jakob PM. Dynamic autocalibrated parallel imaging using temporal GRAPPA (TGRAPPA). Magnetic resonance in medicine : official journal of the Society of Magnetic Resonance in Medicine / Society of Magnetic Resonance in Medicine 2005;53:981-5.
Figures