2952
Patterns of myocardial strain are unique in HIV+ patients with heart failure with preserved ejection fraction1Radiology, Northwestern University, Chicago, IL, United States, 2Medicine - Cardiology, Northwestern University, Chicago, IL, United States
Synopsis
Human immunodeficiency virus (HIV) infection is associated with impaired cardiac function beyond what is expected from coronary artery disease alone. Our aim in the current study was to compare myocardial strain in a cohort HIV+ patients and uninfected controls with adjudicated heart failure (HF) using cardiovascular MRI feature tracking. Our results demonstrate unique Ecc and Err strain patterns in HIV+ patients, with relative apical sparing in HIV+ patients with EF>50%, but relative mid-LV and global strain reduction in HIV+ patients with EF<50%. This constellation of findings suggests that patterns of myocardial functional impairment may be unique in HIV+ HF patients.
Introduction
Human immunodeficiency virus (HIV) infection is associated with impaired cardiac function and myocardial fibrosis beyond what is expected in the setting of coronary artery disease alone for reasons that are incompletely understood. Prior studies have demonstrated that myocardial strain is impaired in otherwise healthy HIV+ patients (1) and late gadolinium enhancement (LGE) is increased relative to non-HIV patients even when controlling for coronary artery disease in this group.(2) Patients with chronic HIV are now living significantly longer due to improvement in treatment and monitoring, and risks for cardiovascular diseases including myocardial infarction and heart failure appear to be elevated among HIV-infected patients. Myocardial strain can be calculated from steady state free precession (SSFP) images using feature tracking analysis software, and has been used to quantify myocardial strain in multiple cardiomyopathies. (3) Our aim in the current study was to compare regional and global strain in a cohort HIV+ patients and uninfected controls with heart failure (HF).Methods
Subjects were drawn from an electronic cohort (HIVE-4CVD) which includes HIV+ patients and uninfected controls matched for demographics and zip code in a 1:2 ratio. This retrospective, nested study within HIVE-4CVD included 35 HIV+ subjects (Age: 49 ± 13 years-old, 28:7 M:F) and 21 uninfected controls (Age: 50 ± 14 years, 18:3 M:F) who 1) had adjudicated heart failure, and 2) had clinically indicated CMR. Heart failure adjudication was performed for all subjects in the HIVE-4CVD cohort by two independent physicians. In all patients in the current study, balanced SSFP, ECG-gated cine MRI in short axis was performed at the base, mid, and apex and in the 4-chamber orientation (spatial resolution: 1.4-2.0 x 1.4-2.0 x 6-8 mm3, TR: 32-68 ms, TE: 1.1-1.5 ms, flip angle: 54-80o). Ejection fraction and regional (base, mid, apex) and global strain were evaluated from the cine images using dedicated software (cvi42, Circle Cardiovascular Imaging, Inc., Calgary, Canada). Peak circumferential (Ecc) and radial (Err) strain were calculated at each slice for regional strain assessment and then averaged to obtain global peak strain values. Global longitudinal strain (GLS) was measured from the 4-chamber images. Initial comparisons were performed between HIV- and HIV+ patients. Subgroup comparisons were performed between patients with preserved ejection fraction (EF), defined as EF ≥ 50% (HIV+: n = 10, HIV-: n = 8), and patients with EF < 50% (HIV+: n = 25, HIV-: n = 13). All between groups were performed with a t-test and α = 0.05.Results
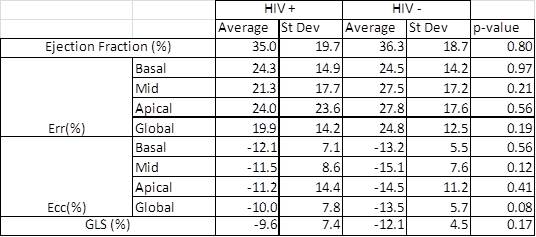
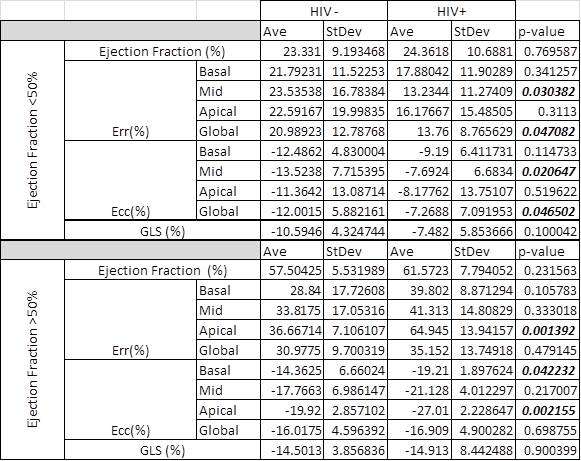
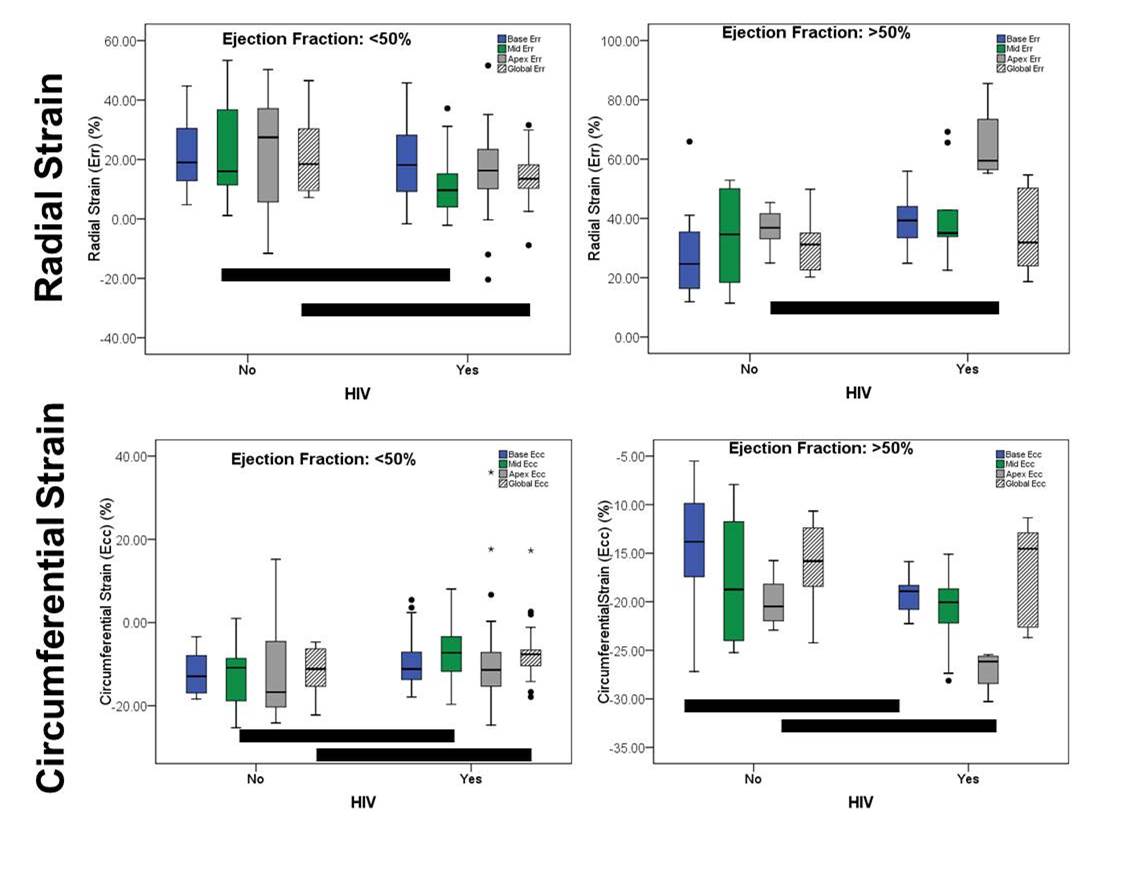
The performance of the feature tracking software was relatively poor at the apex, resulting in no apical strain data in 10 HIV+ patients and 3 HIV- patients. These patients were excluded from apical strain comparisons. Base and mid-short axis Err and Ecc were calculated for all patients. Comparing HIV+ and HIV- patients, there is no significant difference in EF, regional Err and Ecc, global Err and Ecc, or GLS (Table 1). On subgroup analysis, there was no significant difference in EF within either subgroup. HIV+ patients with EF>50% demonstrated relatively higher magnitude basal Ecc and apical Err and Ecc (Table 2), suggesting relative sparing of the apex which is more pronounced than HIV- patients (Figure). In patients with EF<50%, HIV+ patients had relatively reduced magnitude global and mid-short axis Ecc and Err (Table 2).Conclusions
In patients with adjudicated heart failure, there were no differences in global or regional myocardial strain for HIV-infected versus uninfected patients. However, when stratifying patients by ejection fraction, unique Ecc and Err strain patterns are present in HIV+ patients. In this analysis, there was relative apical sparing in HIV+ patients with EF>50%, but relative mid-LV and global strain reduction in HIV+ patients with EF<50%. This constellation of findings suggests that patterns of myocardial functional impairment may be unique in HIV+ HF patients. Future work will include LGE assessment and correlation with epicardial coronary artery disease to further refine CMR myocardial function and tissue characterization parameters in this cohort. We plan to correlate these features with cardiovascular outcomes with the ultimate goal of improved risk-stratification in HIV+ HF patients.Acknowledgements
No acknowledgement found.References
1. Holloway CJ, Ntusi N, Suttie J, et al. Comprehensive cardiac magnetic resonance imaging and spectroscopy reveal a high burden of myocardial disease in HIV patients. Circulation 2013;128(8):814-822. 2. Feinstein MJ, Mitter SS, Yadlapati A, et al. HIV-Related Myocardial Vulnerability to Infarction and Coronary Artery Disease. J Am Coll Cardiol 2016;68(18):2026-2027.
3. Scatteia A, Baritussio A, Bucciarelli-Ducci C. Strain imaging using cardiac magnetic resonance. Heart failure reviews 2017;22(4):465-476.
Figures