2951
The right ventricular deformation in type 2 diabetes mellitus patients: insights from cardiac magnetic resonance feature-tracking1Department of Radiology, West China Hospital, Sichuan University, 37# Guo Xue Xiang, Chengdu, Sichuan 610041, China., Chengdu, China, 2Department of Radiology, West China Second University Hospital, Sichuan University, 20# Section 3 South Renmin Road, Chengdu, Sichuan 610041, China., Chengdu, China
Synopsis
Aim of this study was to clarify the feasibility of cardiovascular magnetic resonance (CMR)-derived feature-tracking for assessing right ventricle (RV) myocardial deformation in patients with type 2 diabetes mellitus (T2DM). Seventy T2DM patients and 22 healthy controls were enrolled. Cardiac volumes and function, and RV tissue-tracking parameters were determined by CMR. Compared with healthy subjects, significantly lower values of some global and regional strain parameters in T2DM (all p<0.05). Our results concluded that abnormal RV myocardial deformation could be monitored using CMR feature-tracking in T2DM; and the systolic and diastolic dysfunction was associated with RV volumes, HDL, and HbA1c.
Introduction
Clinically, assessment of myocardial function is essential in patients with type 2 diabetes mellitus (T2DM) to predict outcome and determine therapeutic method. Aim of this study was to clarify the feasibility of cardiovascular magnetic resonance (CMR)-derived feature tracking for assessing right ventricle (RV) myocardial deformation in T2DM.Methods
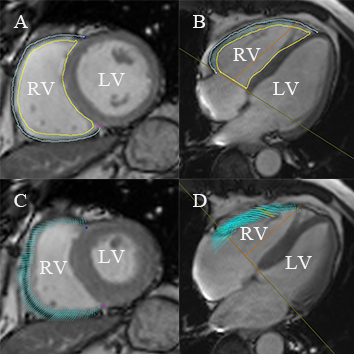
Seventy T2DM patients and 22 healthy controls were enrolled. Cardiac volumes and function, and RV tissue tracking parameters [the global and regional longitudinal, circumferential, and radial peak strain, peak diastolic strain rate (PDSR), and peak systolic strain rate (PSSR)] were determined by CMR. Pearson’s correlation was used to evaluate relationships between RV tissue tracking parameters with the cardiac volumes, function, and biomarkers. The intraclass correlation coefficient (ICC) was used to evaluate the inter- and intra-observer variability.Results
Compared with healthy subjects, significantly lower values of global longitudinal and circumferential PS in the T2DM (-10.72% vs. -6.96%; p<0.001; and-4.24% vs -2.39%; p=0.001, respectively) and the circumferential PSSR decreased significantly (p=0.001). Furthermore, in comparison with healthy controls, the regional strain abnormalities in T2DM patients were mainly involved in the mid-ventricular segment of longitudinal, circumferential and radial PS (-10.90% vs. -6.84%; p<0.05; -7.26% vs. -3.59%; p<0.01; and 27.45% vs. 21.29%; p<0.05; respectively). In the T2DM cohort, longitudinal PS correlated with RV end-diastolic volume (EDV), RV end-systolic volume (ESV), and radial PS correlated to RV EDV, RV ESV, high-density lipoprotein (HDL), and glycosylated hemoglobin (HbA1c) (all P<0.05). The ICCs for intra- and inter-observer variability were 0.798–0.905 and 0.701–0.897.Discussion
The main findings of our study are that in T2DM patients, 1) the impairment of RV function encompasses both diastolic and systolic abnormalities, and 2) deterioration in right ventricular performance was evidenced by tissue tracking parameters in multi-dimensional directions, and 3) for the regional strain abnormalities, mid-ventricular segments were mainly involved in.
The present study, based on the quantitative estimation of global and regional deformation parameters in multi-dimensional directions using CMR feature tracking, revealed both systolic and diastolic RV dysfunction in T2DM, which was different from several studies that RV systolic function remained preserved in diabetes patients [1] and was in line with a previous ultrasonic strain/strain rate study [2]. The PS and PSSR, markers of regional contractile function, were both reduced in global and regional parameters. The PDSR, reflecting local relaxation of cardiac muscle, was also reduced in regional strain indexes. The deterioration of RV performance in the mid-ventricular segments was demonstrated in all three directions. The apical segments regional strain anomalies were only shown in the longitudinal direction. However, circumferential strain parameters in the basal segments were significantly higher than control subjects.
Embryological and anatomical evidence suggest that the RV could be divided into three components [3]. Different components of the RV had significant regional differences in the extent of fibers shortening, timing of the contraction–relaxation sequence and the contribution to global RV systolic function [4]. we may speculate the above-mentioned differences shown in our T2DM cohort were related to regional inhomogeneity of the RV, and the circumferential basal segments strain might be explained by the compensation.
Significant relationships between the measures of RV strain and HbA1c was demonstrated in our study, which was in accordance with previous studies [5,6]. Besides, the significant correlations between RV strain parameters and RV volumes and HDL was also being observed. Our findings may be reminding us that well blood glycose and lipid control may be beneficial for RV function preserved.
Conclusion
In adults with T2DM, abnormal RV myocardial deformation can be monitored using CMR feature-tracking; and the systolic and diastolic dysfunction was associated with RV volumes, HDL, and HbA1c.Acknowledgements
None.References
[1] Tadic M, Ivanovic B, Cuspidi C. Metabolic syndrome and right ventricle: an updated review. Eur J Intern Med. 2013;24(7):608-16.
[2] Kosmala W, Przewlocka-Kosmala M, Mazurek W. Subclinical right ventricular dysfunction in diabetes mellitus--an ultrasonic strain/strain rate study. Diabet Med. 2007;24(6):656-63.
[3] Haddad F, Hunt SA, Rosenthal DN, Murphy DJ. Right ventricular function in cardiovascular disease, part I: Anatomy, physiology, aging, and functional assessment of the right ventricle. Circulation. 2008;117(11):1436-48.
[4] Geva T, Powell AJ, Crawford EC, Chung T, Colan SD. Evaluation of regional differences in right ventricular systolic function by acoustic quantification echocardiography and cine magnetic resonance imag- ing. Circulation 1998; 98: 339–345.
[5] Fang ZY, Schull-Meade R, Downey M, Prins J, Marwick TH. Deter- minants of subclinical diabetic heart disease. Diabetologia 2005; 48: 394–402.
[6] Vinereanu D, Nicolaides E, Tweddel AC, Madler CF, Holst B. Boden et al. Subclinical left ventricular dysfunction in asymptomatic patients with Type II diabetes mellitus, related to serum lipids and glycated haemoglobin. Clin Sci (Lond) 2003; 105: 591–599.
Figures