2949
Right-ventricular Longitudinal Strain Reference Values of Healthy Volunteers by Age and Gender as Measured with CMR Tissue Tracking1Internal Medicine II, University Hospital of Ulm, Ulm, Germany, 2Medical School of Southeast University, Nanjing, China, 3Cardiology Department, Zhongda Hospital Southeast University, Nanjing, China
Synopsis
Our study measured RV longitudinal strain (RVGLS) by CMR 2D tissue tracking and investigated its diagnostic role in patients with RV heart failure.
150 healthy volunteers in three age groups (G20-40 years, G41-60 years, and G61-80 years) and 30 patients diagnosed as DCM were recruited.
Normal RVGLS was -23.9%±5.2% with significant higher values in females in G41-60 and G61-80. The cut-off value identified as -13.71% showed good sensitivity, specificity, positive and negative predictive value in diagnosing RV contractile dysfunction among DCM patients.
In summary, RVGLS were increased in females, and it benefited the evaluation of RV contractile function.
Introduction
CMR based tissue tracking provides subtle insight into right-ventricular (RV) mechanical function by measuring myocardial strains. Reference values from healthy volunteers without any history of cardiovascular diseases are required as a fundamental step towards clinical routine. In our study, RV longitudinal strain were measured by 2D tissue tracking, followed by investigating age- and gender-related differences as well as diagnostic role in patients with RV heart failure.
Methods
150 healthy volunteers in three age groups (G20-40 years, G41-60 years, and G61-80 years) were recruited continuously, subdivided into males/females with 25 volunteers each. 30 patients diagnosed as dilated cardiomyopathy (DCM), 9 of whom presented abnormal RV ejection fraction (RVEF<40%), were also recruited.
Global peak longitudinal strain was generated by CMR tissue tracking (CVI42, Circle, Calgary, Canada) in standard steady-state free precession (SSFP) cine images acquired at 1.5T. RV myocardial contours were delineated in short-axis stack and 2-chamber long-axis cine images.
Results
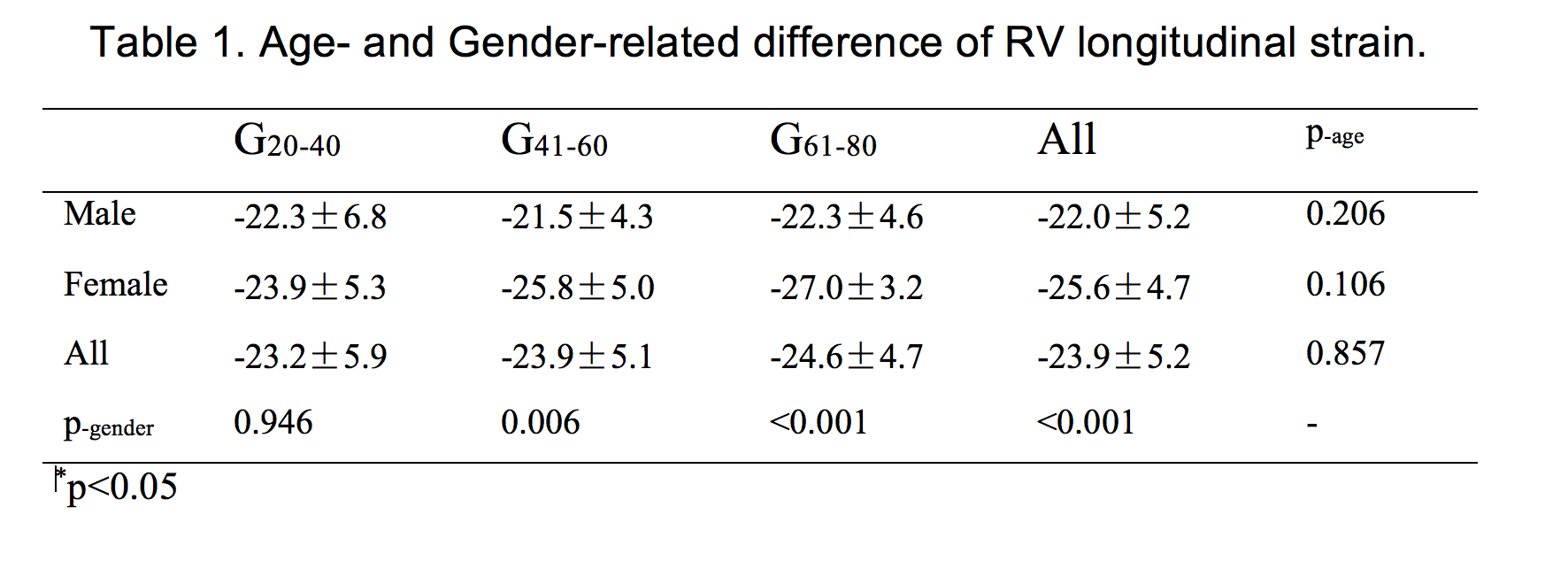
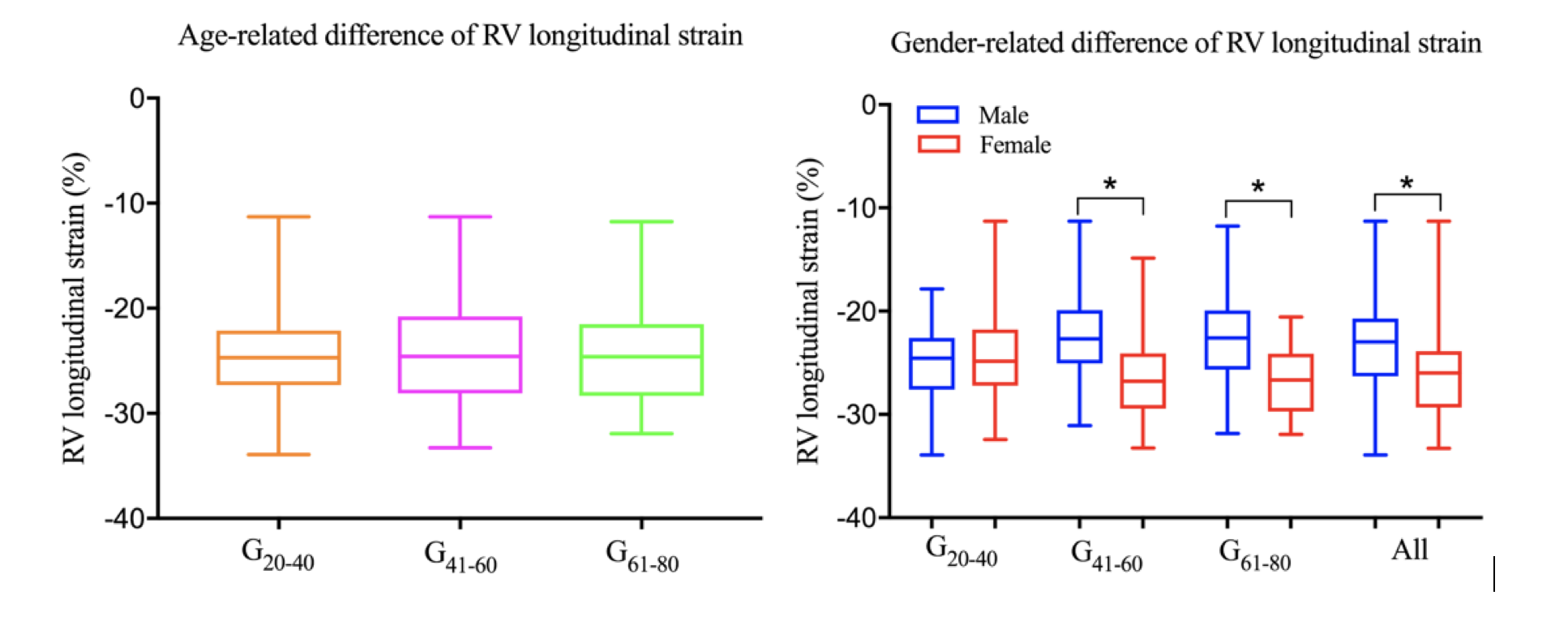
RV global longitudinal peak strain (Table 1 & Figure 1) in the whole healthy cohort was -23.9%±5.2%. Strain values were -23.2%±5.9% for G20-40, -23.9%±5.1% for G41-60, and -24.6%±4.7% for G61-80 age group, implying no significant age-related difference in RV longitudinal shortening. However, females showed more powerful longitudinal shortening and significantly higher longitudinal strain values compared to males in G41-60 and G61-80.
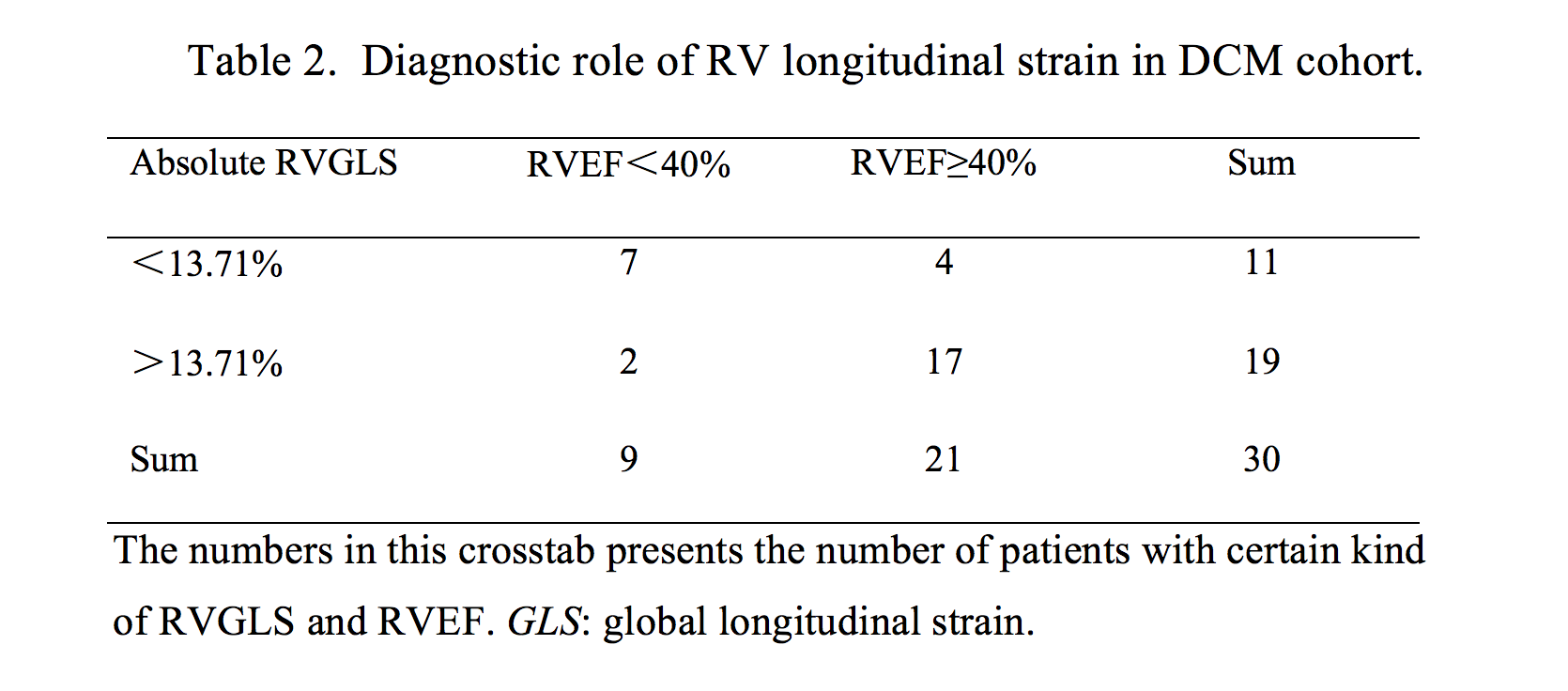
From the healthy volunteer data, the cut-off value (mean value+1.96*standard deviation) of normal RV global longitudinal strain was identified as -13.71%.
In the DCM cohort (Table 2), 19 patients presented higher absolute values than -13.71% (more longitudinal shortening), and 2 of them had abnormal RVEF. 11 patients showed lower absolute values than -13.71% (abnormal shortening), while 4 of them had normal RVEF. So the sensitivity and specificity of the cut-off in diagnosing RV contractile dysfunction were 77.8% and 81.0%, positive and negative predictive value were 63.6% and 89.5%, respectively.
Conclusion
In summary, RV global longitudinal peak strains were increased in females, which might be associated with the smaller RV size compared to males and require separate reference values for males/females. Besides, this mechanical parameter seems to play a good diagnostic role on evaluating RV contractile function among DCM patients.Acknowledgements
We acknowledge the technical support by Circle.References
No reference found.Figures