2944
Quantitative phase-contrast CMR of blood flow in fetal vessels gated by Doppler ultrasound: comparison with metric optimized gating1Lund University, Skåne University Hospital, Department of Clinical Sciences Lund, Clinical Physiology, Lund, Sweden, 2Lund University, Skåne University Hospital, Department of Clinical Sciences Lund, Diagnostic Radiology, Lund, Sweden, 3Lund University, Department of Health Sciences, Physiotherapy, Lund, Sweden, 4Lund University, Department of Biomedical Engineering, Faculty of Engineering, Lund, Sweden, 5Department of Diagnostic and Interventional Radiology, University Medical Center Hamburg-Eppendorf, Hamburg, Germany, 6northh medical GmbH, Martinistraße 52, 20246, Hamburg, Germany, 7Laboratory of Computing, Medical Informatics and Biomedical – Imaging Technologies, Aristotle University of Thessaloniki, School of Medicine, Thessaloniki, Greece
Synopsis
The recent Doppler UltraSound (DUS) triggering method, which utilizes an MR-compatible ultrasound device to assess fetal heart contractions to provide a triggering/gating signal may improve fetal quantitative flow assessment by phase-contrast CMR. We evaluated the DUS method for blood flow measurements in the fetal descending aorta and umbilical vein, in comparison with the metric optimized gating method. Fetal quantitative blood flow by phase-contrast CMR is feasible using the DUS method. This further increases usability of fetal CMR, as post-processing is not needed.
BACKGROUND
Fetal cardiovascular magnetic resonance (CMR) imaging is increasingly applied in challenging clinical cases of cardiac malformation and for fetal cardiovascular research. Quantitative phase-contrast (PC) CMR is hampered by the fact that there is currently no solution for acquiring the fetal electrocardiogram for triggering. The metric optimized gating (MOG) post-processing method1,2 combines oversampling of each heartbeat with retrospective numerical optimization to sort the acquired data and can be considered the current fetal CMR gold standard for quantitative flow. A recent suggestion to overcome time-consuming post-processing for fetal flow quantification is the Doppler UltraSound (DUS) triggering method (sMaRT-sync, northh medical GmbH), which utilizes an MR-compatible ultrasound device to assess fetal heart contractions to provide a triggering / gating signal as input for the MR scanner. This method has been validated to ECG-gated phase-contrast flow measurement in the adult aorta,3 but not previously applied for human fetal phase-contrast CMR blood flow measurements.
The aims of the current study were therefore to evaluate the DUS method for fetal quantitative blood flow in the fetal descending aorta and umbilical vein, and to compare this method with the MOG method.
METHODS
The regional ethics board approved the study. Written informed consent was obtained from six pregnant women (age 26–34 years) with singleton fetuses (gestational week 34–38).
Cardiac magnetic resonance imaging was performed at 1.5 T (MAGNETOM Aera, Siemens Healthcare GmbH, Erlangen, Germany) using a combination of an 18-channel phased array and a dedicated spine receiver coil. Phase-contrast quantitative flow images (TR/TE=5.1/2.8ms, flip angle 20°, matrix 256, 1.3×1.3×5mm3, Venc 150cm/s) of the fetal descending aorta (n=6) and umbilical vein (n=4) were acquired in a randomized order using both the metric optimised gating (MOG) and Doppler UltraSound (DUS) methods. Metric optimized gating images were reconstructed using the MOG-Public Software (version 2.7; https://github.com/MetricOptimizedGating/MOG-Public). Phase-contrast CMR images were analyzed in Segment (version 2.0; Medviso AB, Lund, Sweden) for quantitative measurements.4 Two blinded expert observers (17 and 12 years of CMR experience) independently evaluated the images. Interobserver variability was based on each observer’s first measurement, and both intra- and interobserver and intermethod variability were assessed according to Bland-Altman.5
RESULTS
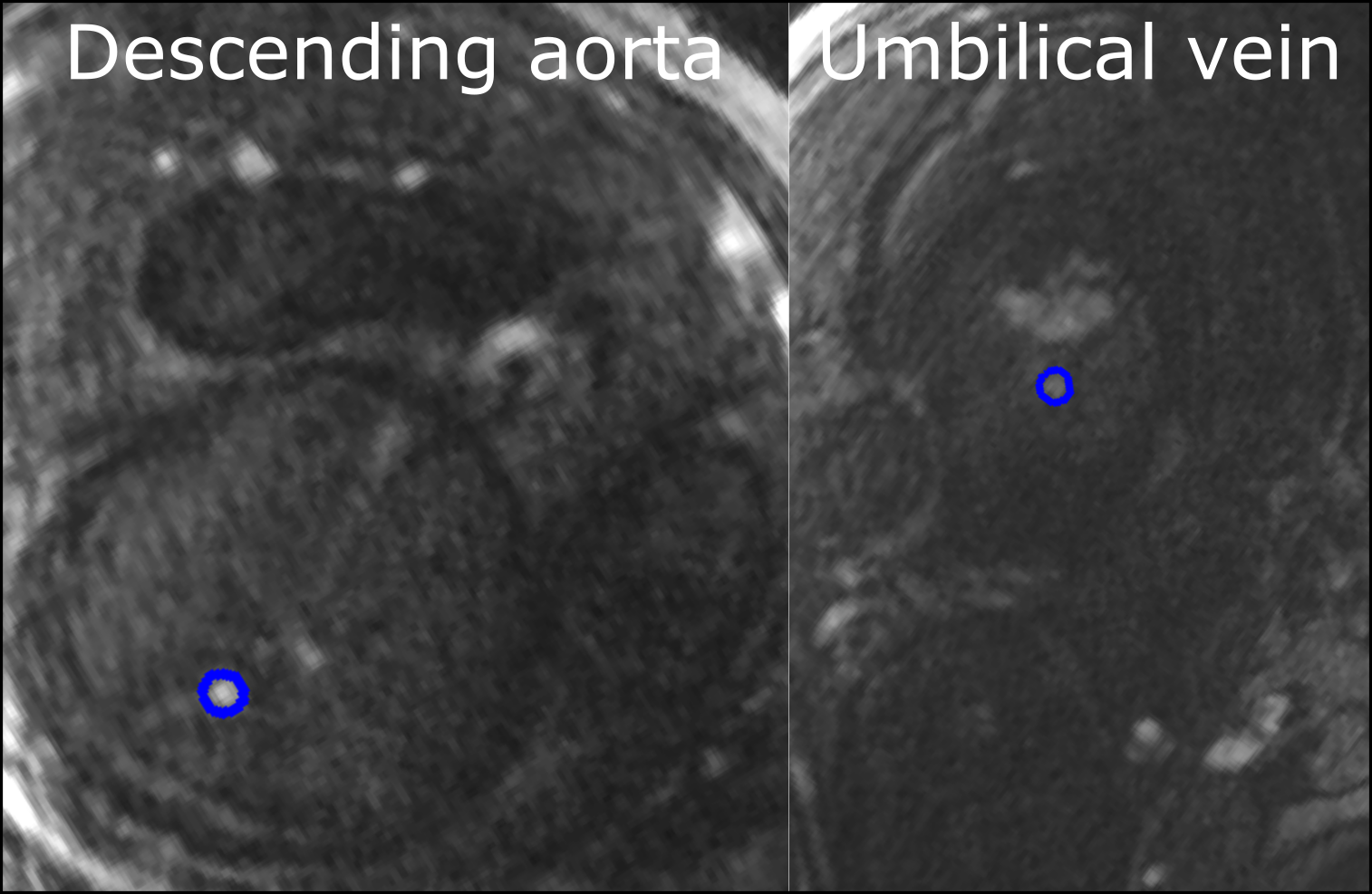
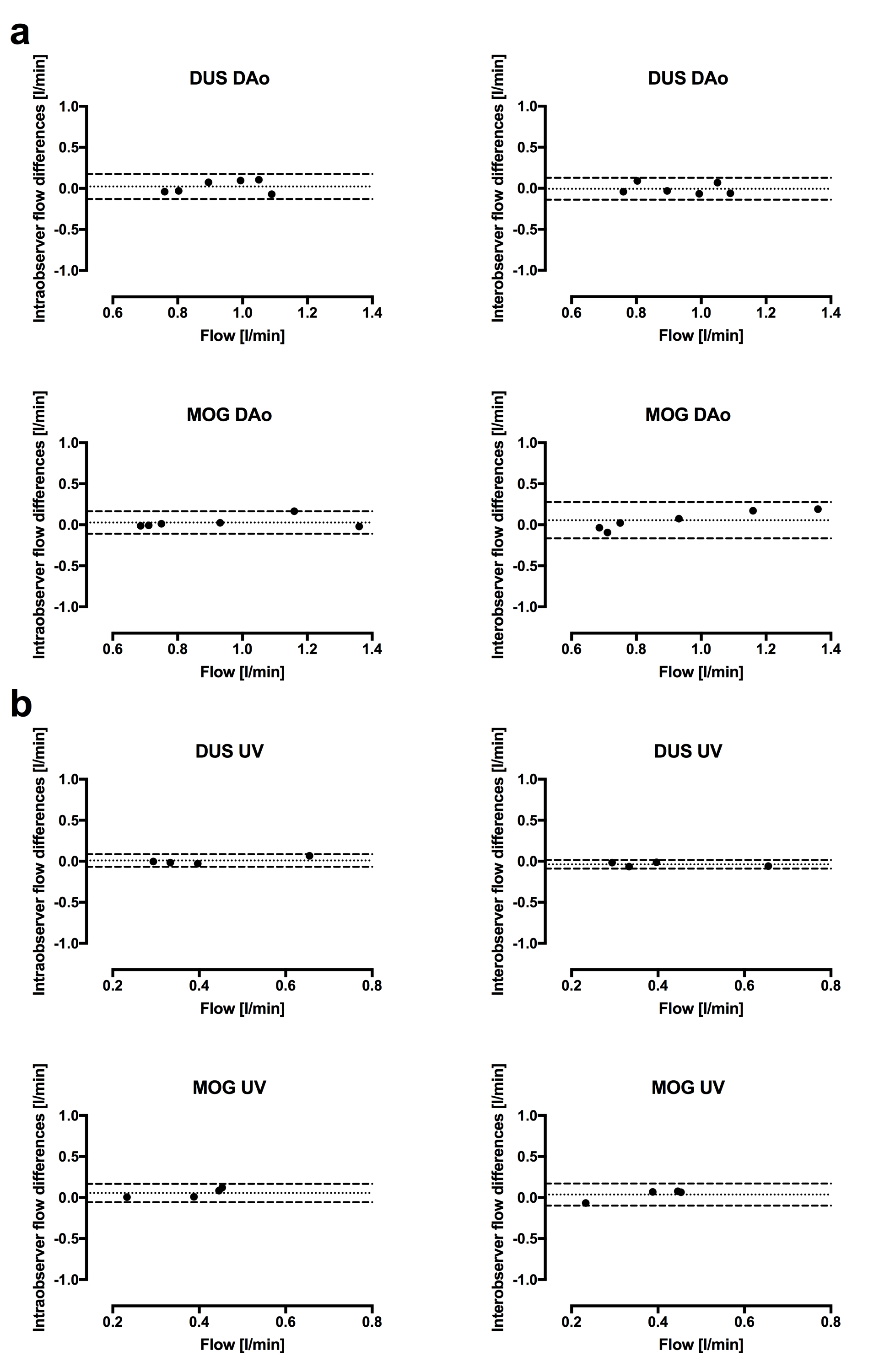
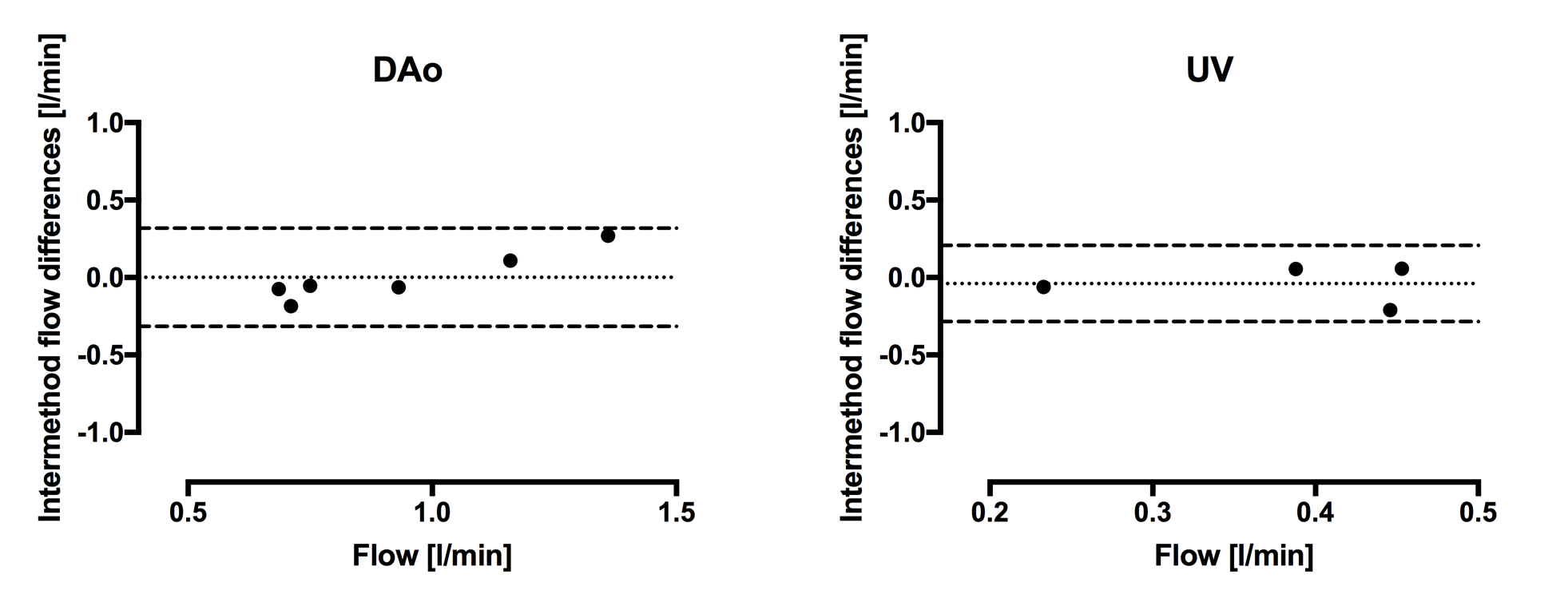
Adequate gating signal by the DUS device was continuous for approximately 40 minutes in all cases but one, in which the fetus turned from left to right requiring repositioning of the device. Representative image quality and delineations of the fetal descending aorta and umbilical vein are presented in Figure 1. The fetal descending aorta was 5-7 mm with quantitative flow 0.9±0.3 l/min by MOG. Pulsatility was shown for the fetal descending aorta after MOG reconstruction in all cases. Using the DUS method, intra- and interobserver variability were for the fetal descending aorta 0.02±0.08 l/min and 0.01±0.07 l/min. Using the MOG method, intra- and interobserver variability were 0.03±0.07 l/min and 0.06±0.11 l/min, respectively (Figure 2). Bias and variability between DUS and MOG for the fetal descending aorta was 0.00±0.16 l/min (Figure 3).
For the umbilical vein, diameters were 5-9mm with quantitative flow 0.5±0.2 l/min by MOG. Using the DUS method, intra- and interobserver variability were for the umbilical vein 0.01±0.04 l/min and 0.04±0.03 l/min. Using the MOG method, intra- and interobserver variability were 0.06±0.06 l/min and 0.04±0.07 l/min, respectively (Figure 2). Bias and variability between DUS and MOG for the umbilical vein was 0.04±0.13 l/min (Figure 3).
CONCLUSIONS
Fetal quantitative blood flow by phase-contrast CMR is feasible using the DUS method. This further increases usability of fetal CMR, as post-processing is not needed. However, MOG remains useful in cases of fetal motion where DUS potentially may be inconclusive. To be considered in future studies, it should be noted that with current fetal PC-CMR sequences and reconstruction methods at 1.5T, accuracy might be limited by the signal-to-noise ratio independent of gating method used.Acknowledgements
Funding was provided by the Swedish Heart and Lung Foundation, the Skåne University Hospital and by the Medical Faculty at Lund University.References
[1] Jansz MS et al. MRM (2010).
[2] Bidhult SL et al. ISMRM (2017).
[3] Kording F et al. Magn Reson Med Sci (2017).
[4] Heiberg E et al. BMC Med Imag (2010).
[5] Bland & Altman. Lancet (1986).
Figures