2941
Hemodynamic Evaluation in Patients with Tetralogy of Fallot after Operation: Repeatability And Internal Consistency of 4D Flow and 2D Phase Contrast by Cardiovascular Magnetic Resonance1Radiology, Shanghai Children's Medical Center, Shanghai, China, 2MR Research GE Healthcare, Shanghai, China
Synopsis
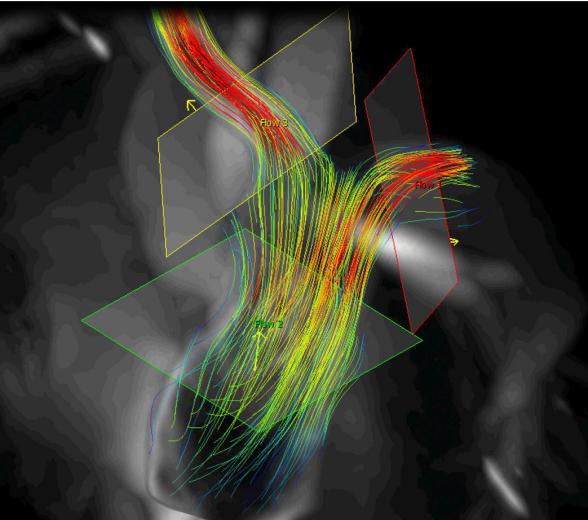
4D flow MRI offers the ability to measure and visualize the temporal evolution of complex blood flow patterns within an 3D volume. Some studies have been performed to validate 4D PC flow measurements, such as the comparison of 4D PC flow measurements to two-dimensional (2D) flow and to phantoms measurements as a reference standard. We hypothesized that 4D flow could be used to evaluate the hemodynamic parameters in patients with tetralogy of Fallot compare with 2D flow.
Purpose:
The aim of this study was to compare flow and velocity quantification of pulmonary arteries by 4D flow and 2D phase contrast (PC) cardiovascular magnetic resonance(CMR) in patients with Tetralogy of Fallot(ToF) after operation compared with healthy volunteers.Methods:
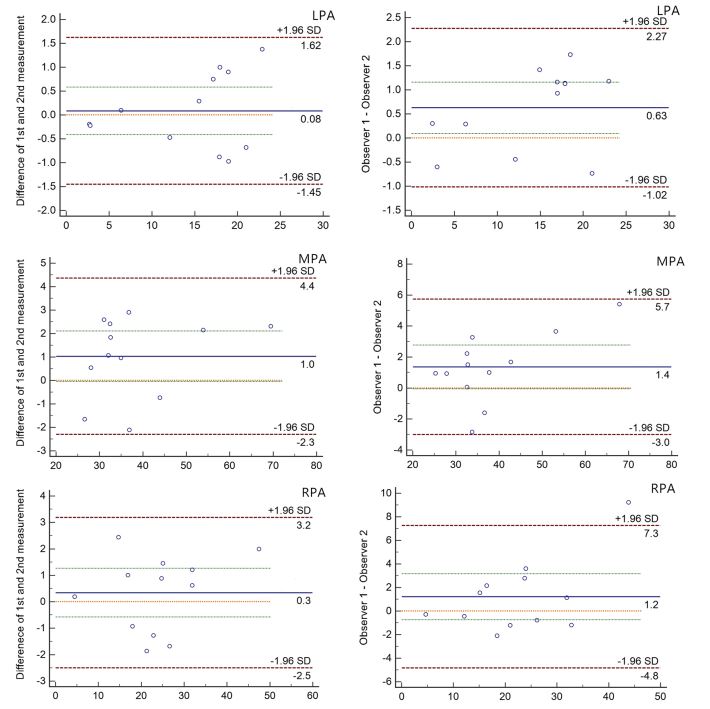
12 patients (mean age 11.75±2.73 years, follow-up duration:6-13 years) with ToF after surgery and 8 age-matched healthy children volunteers were included in this retrospective study. The patient and control group underwent 4D flow and 2D PC sequence. CMR imaging was conducted on a 3.0 Tesla whole-body scanner (Discovery MR 750, GE, USA) using a 8-channel phased-array cardiac coil. The whole heart 4D flow CMR was performed (spatial resolution=1.2-1.6×1.2-1.6×2.0-2.4 mm3 , FOV=340×340 mm2 , slab thickness=55-75 mm, temporal resolution=34.4 ms, TE=2.1 ms, TR=4.3 ms, flip angle=8-12°, bandwidth=62.5 Hz/pixel, velocity sensitivity=160 cm/s) with coronal position coverage of the pulmonary arteries. The average scan time was 5-7 min. 4D flow MRI data was preprocessed to correct for noise, eddy currents, maxwell terms, and velocity aliasing using an post-processing software (CVI, Circle, Canada). The pulmonary arteries were measured plane with 4D flow and 2D PC CMR including main pulmonary arteries, left pulmonary arteries, right pulmonary arteries. Blood flow analyses for the plane included: Net Flow (NF), Peak Velocity (PV), and Regurgitant Fraction(RF). Paired t-test was used to calculate the difference of parameters between 4D flow and 2D PC CMR in two groups, respectively. Bland–Altman method identified possible bias and the limits of agreement with the parameters between two observers in ToF group.Results:
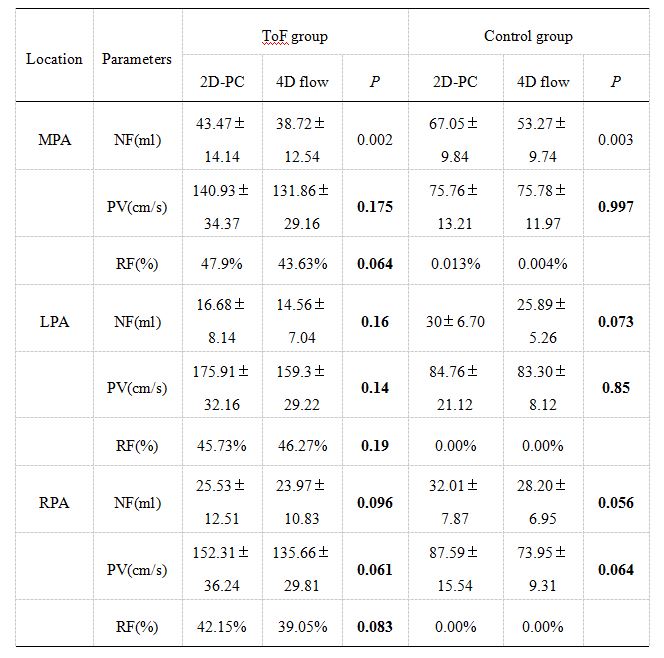
The peak velocity are no significantly difference with 4D flow and 2D PC CMR in the MPA (p = 0.17 for ToF group, p = 0.99 for control group), LPA (p = 0.14 for ToF group, p = 0.85 for control group) and RPA (p = 0.06 for ToF group, p = 0.06 for control group). The Net flow are no significantly difference with 4D flow CMR and 2D PC CMR in the LPA (p = 0.16 for ToF group, p = 0.073 for control group) and RPA (p = 0.06 for ToF group, p = 0.06 for control group) but no in the MPA (p = 0.002 for ToF group, p = 0.003 for control group). The Regurgitation fraction are no significantly difference with 4D flow and 2D PC CMR in MPA, LPA and RPA for ToF group. Bland Altman analysis of blood flow analyses parameters intra- and interobserver reproducibility yielded a good agreement.Conclusions:
4D flow CMR provide an accurate pulmonary blood flow assessment for ToF postoperative patients. Meanwhlie, The 2D and 4D techniques demonstrated strong repeatability of flow measurements in the pulmonary arteries. 4D flow CMR may provide an improved depiction of vessel stenosis compare with 2D PC.Acknowledgements
The authors appreciate Hai-tao You and Tong-tong Han, Circle Imaging Systems, Circle CVI Corporation Canada for technical assistance.References
1. Nordmeyer S, Riesenkampff E, Crelier G, et al. Journal of Magnetic Resonance Imaging, 2010, 32(3): 677-683.
2. Rose M J, Jarvis K, Chowdhary V, et al. Journal of Magnetic Resonance Imaging Jmri, 2016, 44(6):1673-1682.
3. Jarvis K, Vonder M, Barker A J, et al.Journal of Cardiovascular Magnetic Resonance, 2016, 18(1):59.
4. Robinson J D, Rigsby C K, Barker A J, et al. Journal of Cardiovascular Magnetic Resonance, 2014, 16(1):1-2.
Figures