2939
Usefulness of 4D flow in the Diagnosis of Atrial Septal Defects in Adults1Seirei Mikatahara General Hospital, Hamamatsu, Japan, 2Nagoya University, Graduate School of Medicine, Nagoya, Japan, 3Philips Healthcare AsiaPacific, Tokyo, Japan, 4Hamamatsu University School of Medicine, Hamamatsu, Japan
Synopsis
We tested whether 4D flow can offer useful hemodynamic information in the diagnosis of atrial septal defects in Adults. 4D PCA was clearly able to visualize abnormal shunts from the left antrum to the right antrum of ASD patients.
INTRODUCTION
Atrial Septal Defect (ASD) is the most common form of congenital heart disease in adults after bicuspid aortic valve and mitral valve prolapse.The progression is followed by the onset of pulmonary hypertension, arrhythmias, respiratory infections, and other cardiovascular disease. Even a small defect can cause cerebral embolism or cerebral abscess. Transthoracic echocardiography (TTE) is generally used for the diagnosis of ASD; however, angle of field is limited, especially in adults. Transesophageal echocardiography (TEE) is useful; however, relatively invasive.
4D PCA is MR angiography (MRA) postprocessed by combining the magnitude value of x, y z axes, which is automatically produced by 4D Flow data without flow analysis application. Its signal intensity is linear to the velocity of the flowing blood.
The purpose of this study is to test if 4D flow including 4D PCA can offer useful hemodynamic information in patients suspected of having ASDs in Adults
METHODS
Nineteen patients suspected of having ASD underwent cardiac MRI including 4D flow on a wide bore 3.0-T MR scanner. Written informed consent was provided in all cases for this IRB approved study.
Both 4D flow and ECG-gated standard 2D bFFE (CINE) were performed in slices perpendicular to the atrial septum with parameters as follows: For 4D flow, TR (ms)/TE (ms)/FA (degree), 4/2/10; matrix, 256 x 195; reduction factor, 2 - 3; 15–40 slices; 20 phases/cardiac cycle; VENC 250 cm/sec. For CINE, TR (ms)/TE (ms)/FA (degree), 2.4/1.2/50; matrix, 164 x 151; reduction factor, 2.5; slice thickness, 7mm; 20 phases/cardiac cycle.
Two experienced radiologists reviewed both images separately and visually classified into 5 groups (1 definitely absent, 3 probably present, 5 definitely present) in terms of presence or absence of ASD on offline workstation. The evaluation of 4D flow was mainly performed with 4D PCA; however, streamlines and pathlines were also available when necessary.
ROC analysis was performed for each methods of 4D flow and CINE. Final diagnoses of ASD were diagnosed based on cardiac catheter examinations (i.e. O2 step-up ) or intra-operative findings.
RESULTS
Among nine cases finally diagnosed as ASD, eight cases were determined to have ASD by 4D flow and six by CINE. Consequent sensitivities were 0.89 and 0.67, respectively.
Among ten cases finally diagnosed to have no ASD, seven cases were correctly determined to have no ASD by 4D flow and five by CINE. The resultant specificities were 0.70 and 0.50, respectively.
AUCs of ROC analysis were 0.948 and 0.791 for 4D flow and CINE, respectively.
DISCUSSION
In this study, 4D flow showed higher sensitivity and specificity than conventional CINE images.
On the CINE image, when the ASD was large enough, the defect of the septal wall could be clearly depicted; however, it was difficult to detect small ASDs. Conversely, even in cases without ASD, the thin wall portion sometimes looked like ASD because of its low spatial resolution on the CINE images.
On the 4D PCA, the atrial septum could be recognized as the boundary of the signal difference, reflecting the difference in flow velocity between the left and right atria and ASD was visualized as a high intensity jet traversing across the left atrium and the right atrium. By evaluating with streamlines and pathlines in addition to 4D PCA, more detailed observation was possible, and the confidence level increased. We could also quantify the shunt volume quantification using 4D flow data.
As a limitation of streamlines and pathlines utilizing 4D flow data were sometimes misleading depicting false shunting stream across the atrial septum. Thorough observation of 4D PCA was considered priority.
CONCLUSION
4D flow has shown better sensitivity and specificity in detecting ASD as compared with conventional 2DFT cine gradient echo images.Acknowledgements
No acknowledgement found.References
No reference found.Figures
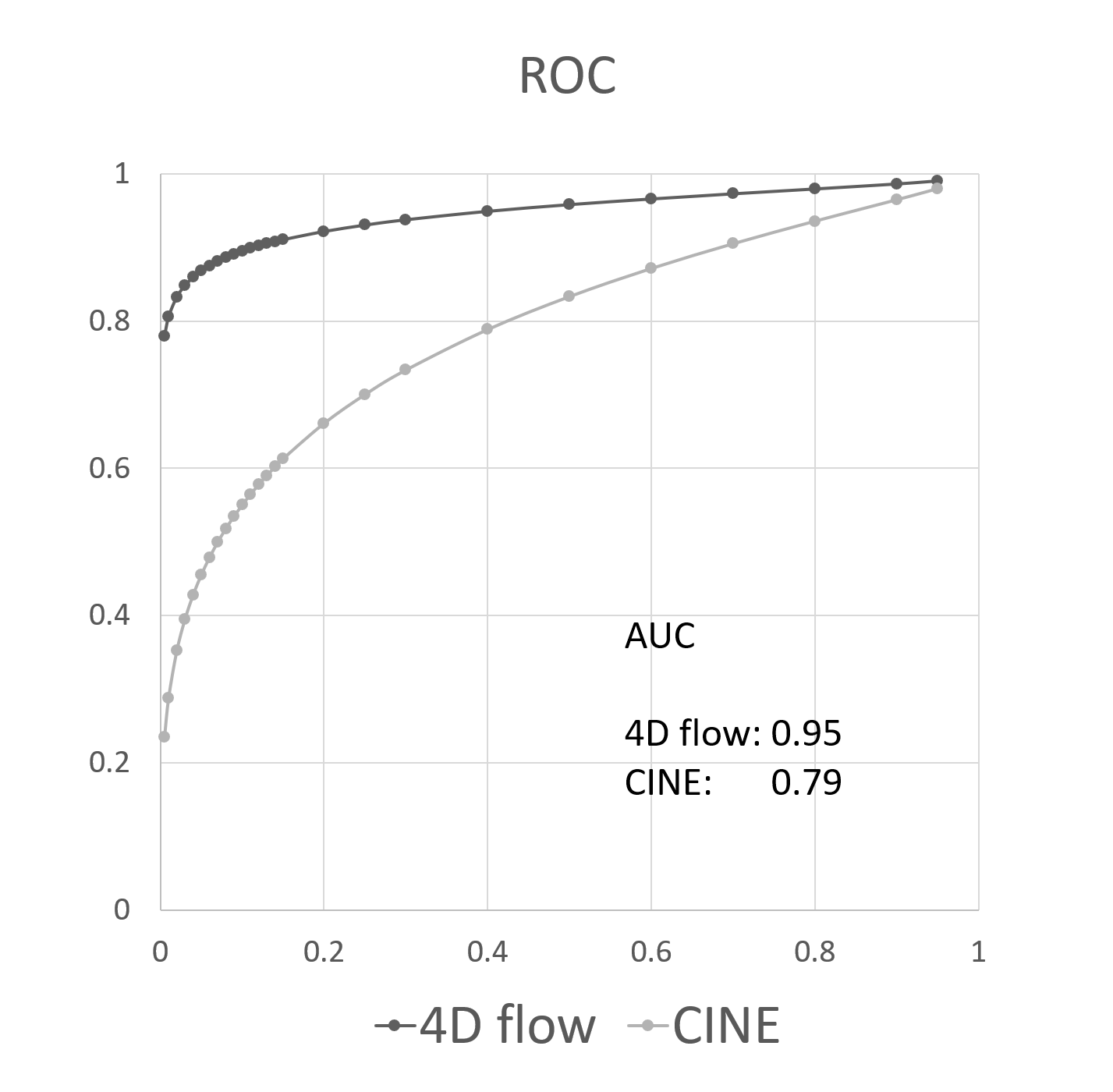
Fig.1
ROC curves of diagnostic performance of ASD either with 4D flow or conventional 2D cine study (CINE). The area under the curve is obviously superior with 4D flow.
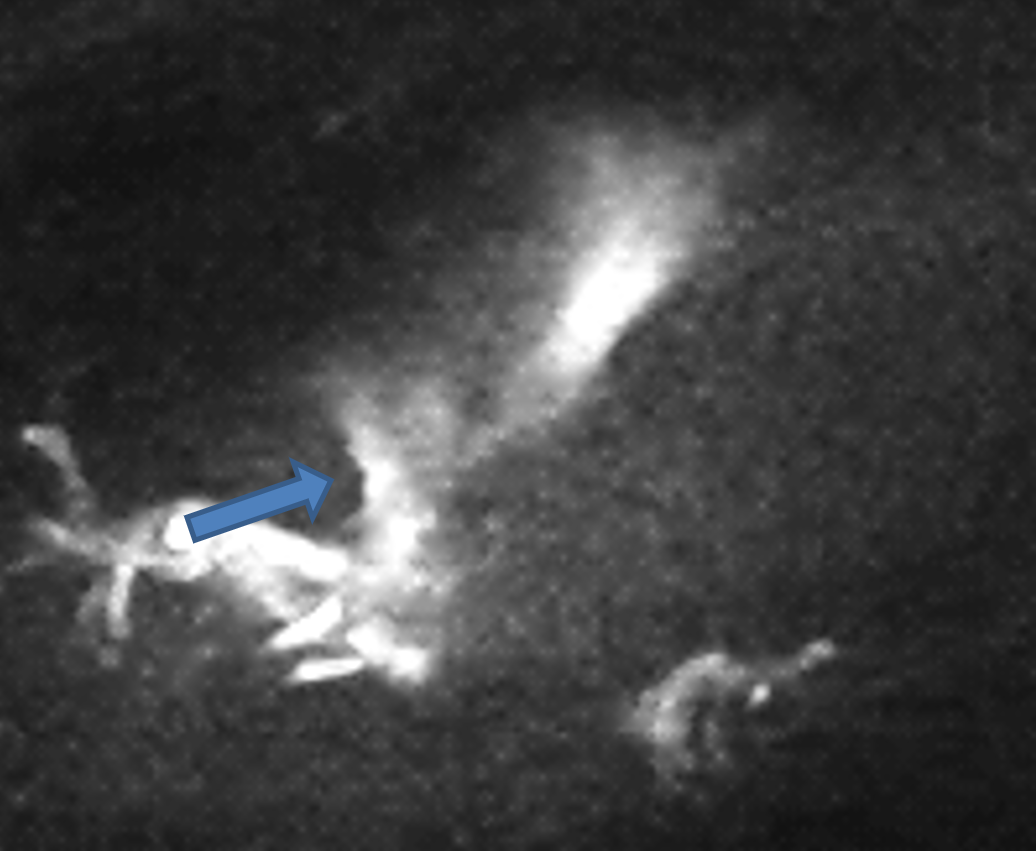
Fig.2
4D PCA depicts a high intensity jet traversing the atrial septum during systole in this representative ASD patient. .
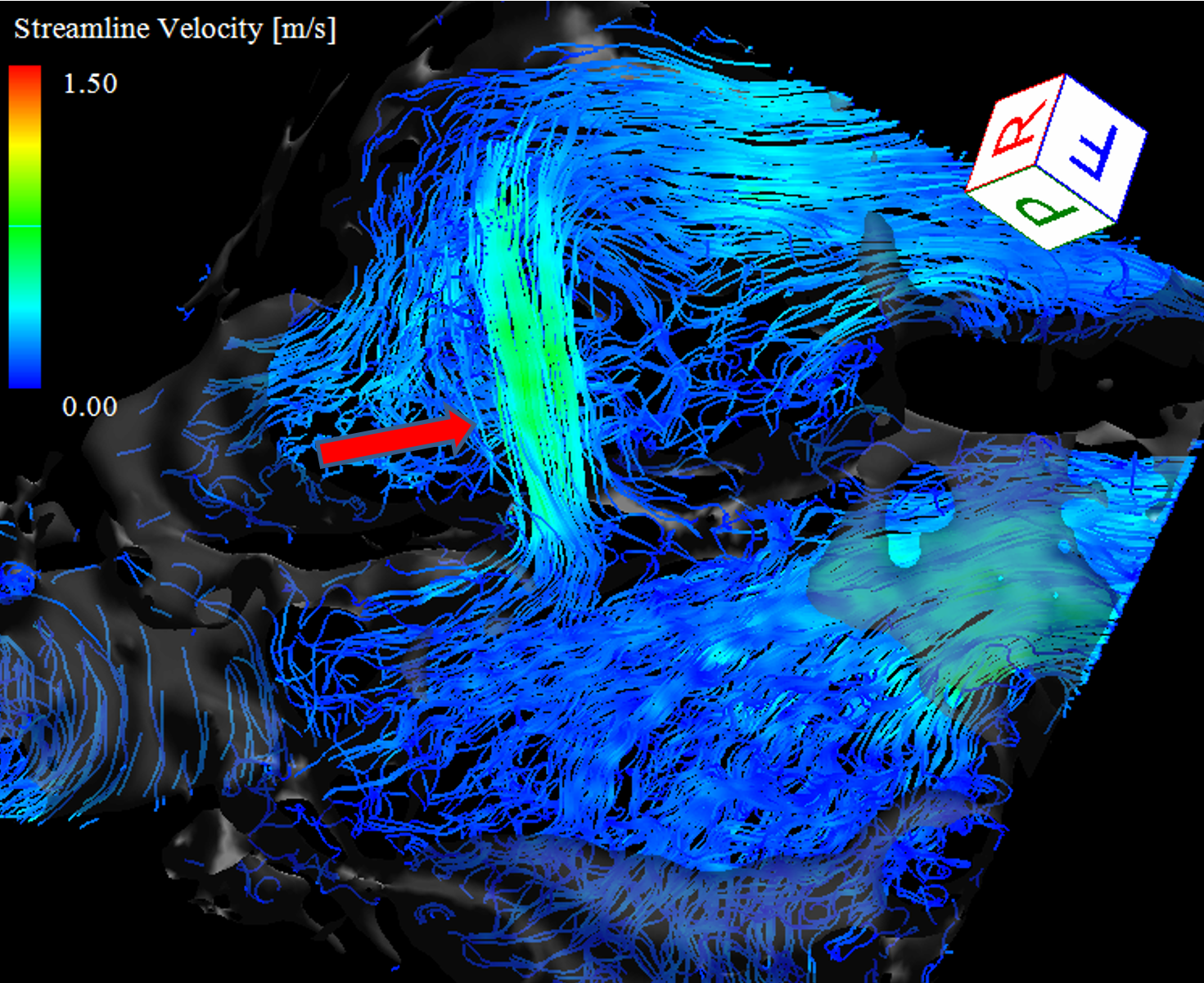
Fig.3
Color coded streamline analysis more clearly visualizes an abnormal shunt flow across the ASD.
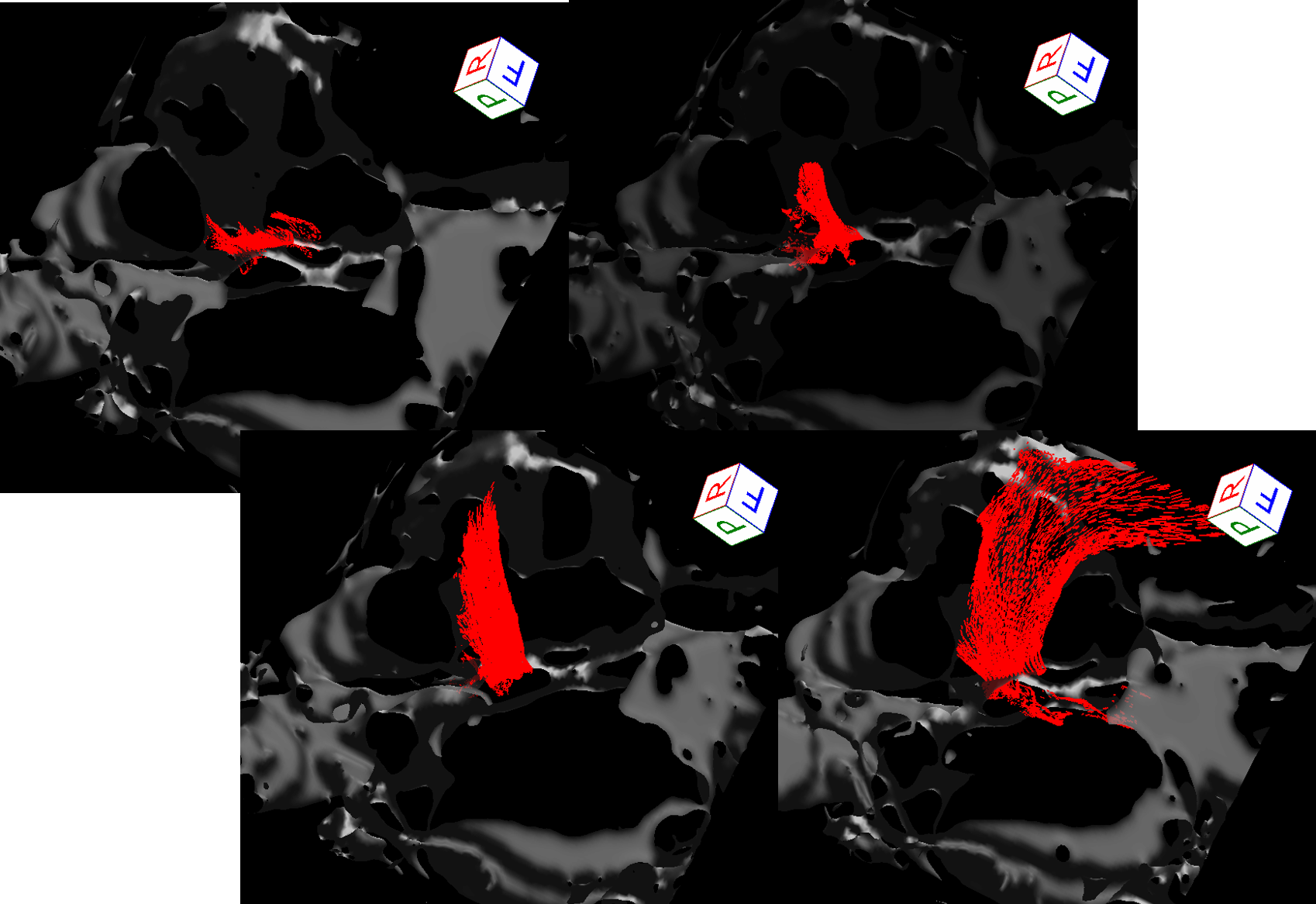
Fig.4
Chronological assessment (i.e., from diastole to systole) of the shunt flow depicted with pathline analysis. Pathline and streamline analysis allow clearer assessment of the shunt flow on condition that the section is properly set at the hole of ASD.