2936
Where phase-contrast measurements should be performed in the presence of stents1GE Healthcare, Munich, Germany, 2Technical University Munich, Munich, Germany, 3German Heart Center, Munich, Germany
Synopsis
Here, a Y-shaped pulsatile flow phantom is used to evaluate the flow quantification error, as measured by 2D CINE PC, caused by magnetic susceptibility in the presence of clinically used MR-conditional ferromagnetic stents, even in ROIs where the artifact is not visualized in magnitude image. Our results indicate that flow measurements should be performed more than 12 mm away from the proximal or distal part of the stent to achieve accurate flow measurements.
Introduction
Accurate velocity and flow quantification using phase-contrast (PC) imaging is of critical interest in cardiac MRI (CMR). One source of quantification error is the magnetic susceptibility caused by the presence of ferromagnetic stents in the different vessels or valves which is very common in CMR patients, even in ROIs where the artifact is not visualized in magnitude image1. Here, we determined flow accuracy in a Y-shaped pulsatile flow phantom with 2 different models of clinical stents and provide guidelines or the proper distance from stent to avoid inaccurate velocity and flow measurements.Methods
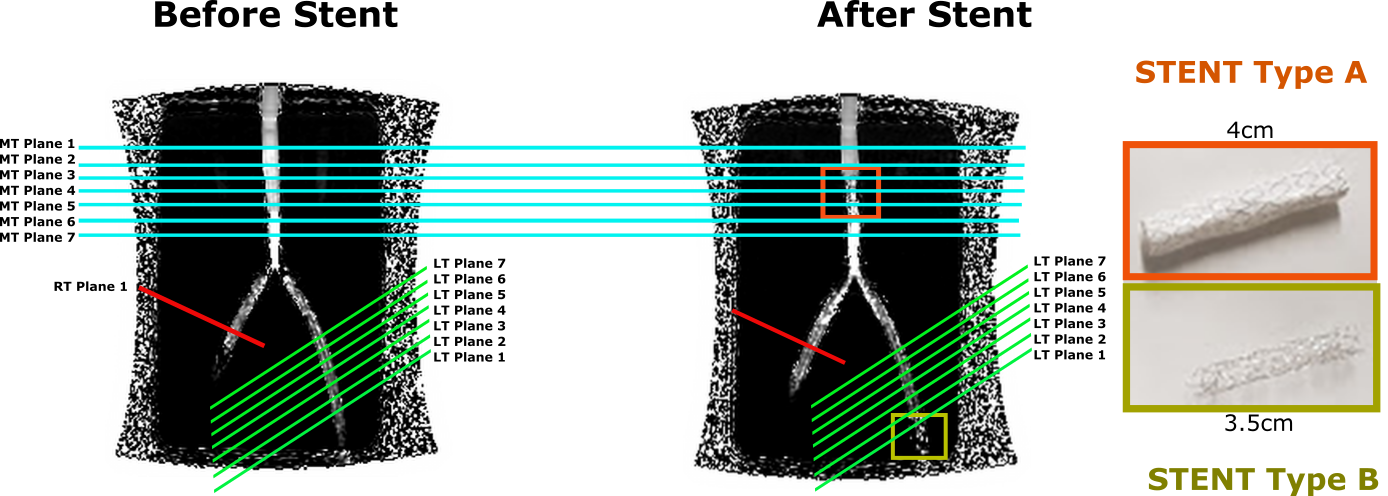
Stents: Two stents, shown in Figure 1 (right), were analyzed. Type A: Lifestream by BARD made of stainless steel fully encapsulated. Type B: Formula 535 by COOK made of 316L stainless steel.
Acquisition: We used a closed-circuit pulsatile flow phantom; composed by an industrial membrane flow pump, an agar box containing three silicone tubes in Y-shaped and a Coriolis flow meter (PROMASS 83F08, Endress+Häuser), to measure a ground-truth net flow value with a precision of ±0.5ml/s. The gating signal was obtained by pulsioxymetry in the inflow tube. Flow phantom scans were performed on a GE 3.0T MR750w (Waukesha, WI). Retrospective gating; “breath-hold” and “free-breathing” (4 averages) 2D through-plane CINE PC were scanned twice per plane at HR 80 using the main parameters defined in Table 1. Measurements were repeated under 4 conditions in each acquisition: before and after placing the stents and with pump ON and OFF. Seven parallel planes were scanned on each tube where stent was going to be placed and one plane in the third tube. Scanned planes are shown in Figure 1.
Analysis: PC net flow measurements were evaluated using cmr42 (Calgary, Canada). Background phase correction (BPC) using static phantom correction (pump OFF) and image-based correction2 was applied. In all cases, the ground-truth value measured by the flow meter was compared to the net flow in the different ROIs in the middle tube (inflow) and to the sum of the right branch tube, where no stent was placed, and the different ROIs in the left branch tubes as measures of accuracy.
Results
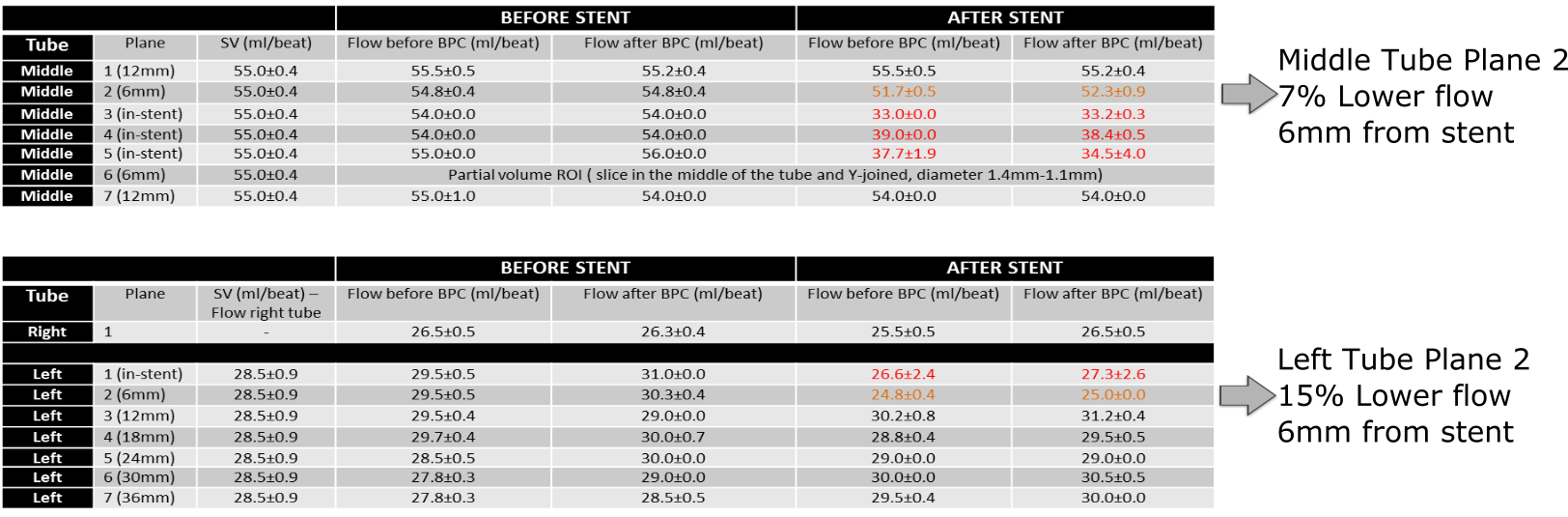
Figure 2 contains all flow measurements for each condition versus the ground-truth net flow as measured by the flow meter (stroke volume). Before placing the stents, all measurements exhibit an error of less than 2% with respect to the ground-truth for both, before and after background phase correction. After stents were placed, it was observed that in-stent flow measurements were completely underestimated by up to 40% which was expected for stainless steel stents1. Moreover, for both stents, the plane situated 6mm away from the stent, where the magnitude image did not show signal loss due to susceptibility, also showed underestimation of the flow of 7% and 15% for the middle tube and left tube, respectively, which is a clinically significant error3. Planes from 12mm away from the stents showed errors of less than 2%. No significant difference was found between static phantom and image based BPC.Discussion
Our results suggest that for two different stainless-steel stents, flow measurements should be performed more than 12 mm away from the proximal or distal part of the stent to achieve accurate flow measurements. These experiments should be extended to the evaluation of the effect in 4DFlow and incorporating platinum or nitinol stents which have shown less dephasing effects in previous studies4,5.Acknowledgements
No acknowledgement found.References
[1] Error Assessment due to Coronary Stents in Flow-Encoded Phase Contrast MR Angiography:A Phantom Study, Lethimonnier et al, JMRI 1999
[2] Nonlinear self-calibrated phase-contrast correction in quantitative cardiac imaging, Tan EK et al, JCMR 2014
[3] Flow measurement by cardiovascular magnetic resonance: a multi-centre multi-vendor study of background phase offset errors that can compromise the accuracy of derived regurgitant or shunt flow measurements, Gatehouse et al, JCMR 2010
[4] Sequential Magnetic Resonance Monitoring of Pulmonary Flow With Endovascular Stents Placed Across the Pulmonary Valve in Growing Swine, Kuehne et al, Circulation 2017
[5] 3.0 T vs. 1.5 T MR Angiography: In Vitro Comparison of Intravascular Stent Artifacts, Wall et al, JMRI 2005
Figures