2911
Multi-Parametric Cardiac MRI is Needed for Accurate Staging of Reperfused Hemorrhagic Myocardial Infarctions1Pacific Theatres Suite 400. 8700 Bevely Boulevard, Cedars-Sinai Medical Center BIRI, Los angeles, CA, United States, 2Dept of Radiology, The First Affiliated Hospital of China Medical University, Shenyang, China, 3Dept of Veterinary Medicine, Louisiana State University, Baton Rouge, LA, Baton Rouge, LA, United States, 4David Geffen School of Medicine, University of California, Los angeles, CA, United States
Synopsis
Cardiac MRI (CMR) based staging of myocardial infarction (MI) with or without contrast agents relies on the resolution of edema in the chronic phase, which is typically determined on the basis of T2-based MRI. However, whether T2 CMR is sufficient for staging all MI types has not been studied. We investigated this using animal models with and without hemorrhagic MIs. Our results show that non-hemorrhagic MIs can be staged based on T2 changes in the MI territory. However, the incomplete resolution of T2 elevations in the peripheral layers of hemorrhagic MI territories can confound staging of hemorrhagic MIs.
Introduction
Cardiac MRI based staging of myocardial infarction (MI) with or without contrast agents relies on the resolution of edema in the chronic phase, which is typically determined on the basis of T2-based imaging. However, whether T2 CMR is sufficient for staging all MI types has not been studied. We hypothesized that prolonged inflammation associated with chronic iron deposits following hemorrhagic MIs promote incomplete resolution of edema in the chronic phase which limit the capability of T2 imaging to stage hemorrhagic MIs.Methods
Hemorrhagic (n=15) and non-hemorrhagic (n=9) MIs were created in dogs following a period of prolonged ischemia followed by reperfusion. Multi-parametric non-contrast mapping (T1, T2 and T2*) and LGE were performed at 1.5T and 3.0T at 5 days (acute) and 8 weeks (chronic) post MI. MR relaxation values and LGE intensities of hemorrhagic, peri-hemorrhagic, non-hemorrhagic and remote territories were measured. Histopathology was performed to elucidate cardiac MRI findings.Results
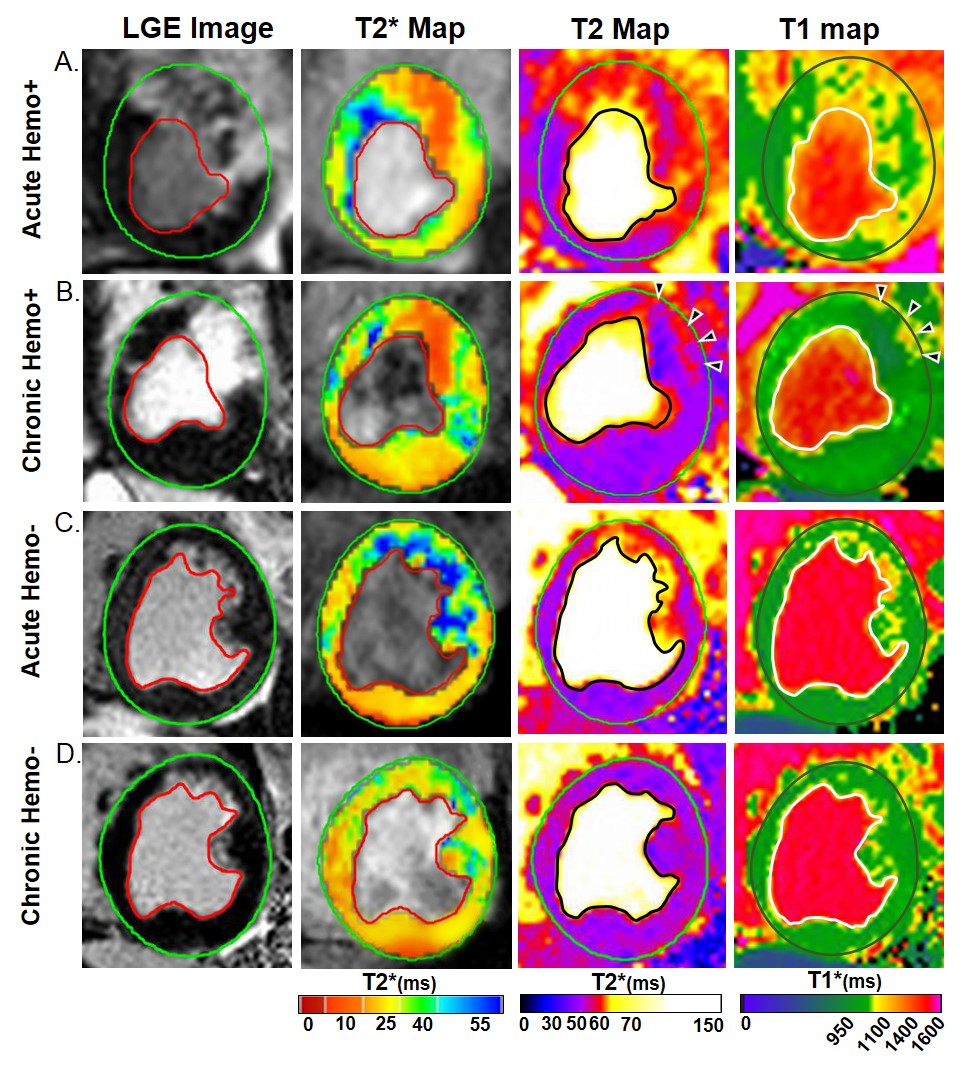
T2 of non-hemorrhagic MIs was significantly elevated in the acute phase relative to remote territories (39.8±12.8%(1.5T) and 27.9±16.5%(3.0T), p<0.0001 for both) but resolved to remote values by week 8 (-0.0±3.2%(1.5T, p=0.678) and -0.5±5.9%(3.0T, p=0.601)). In hemorrhagic MI, T2 of hemorrhage core was significantly elevated in the acute phase (17.7±10.0%(1.5T) and 8.6±8.2%(3.0T), p<0.0001 for both) but decreased below remote values by week 8 (-8.2±3.9%(1.5T) and -5.6±6.0%(3.0T), p<0.0001 for both). In contrast, T2 of the periphery of hemorrhage within MI zone was significantly elevated in the acute phase relative to remote territories (35.0±16.1%(1.5T) and 24.2±10.4%(3.0T), p<0.0001 for both) and remained elevated at 8 weeks post MI (8.6±5.1%(1.5T) and 6.0±3.3%(3.0T), p<0.0001 for both). The observed elevation in T2 in the peri-hemorrhagic zone of MIs and absence of T2 elevation in the non-hemorrhagic MI were consistent with ongoing or absence of histological evidence of inflammation, respectively.Conclusions
Non-hemorrhagic MIs can be staged based on T2 changes in the MI territory. However, the incomplete resolution of T2 elevations in the periphery of hemorrhage associated with ongoing inflammation, well after scar formation, requires additional consideration of the spatial localization of sustained T2 elevations for staging hemorrhagic infarctions.Acknowledgements
This work was supported in part by a grant from NIH ( R01-HL133407)
References
1. Abdel-Aty H, Zagrosek A, Schulz-Menger J, et al. Delayed enhancement and T2 weighted cardiovascular magnetic resonance imaging differentiate acute from chronic myocardial infarction. Circulation 2004;109:2411-6. doi: 10.1161/01.CIR.0000127428. 10985.C6
2. Bulluck H, Rosmini S, Abdel-Gadir A, et al. Residual Myocardial Iron Following Intramyocardial Hemorrhage During the Convalescent Phase of Reperfused ST-Segment-Elevation Myocardial Infarction and Adverse Left Ventricular Remodeling. Circ Cardiovasc Imaging 2016; 9. pii: e004940. doi: 10.1161/CIRCIMAGING.116.004940
3. Kali A, Kumar A, Cokic I, et al. Chronic manifestation of post-reperfusion intramyocardial hemorrhage as regional iron deposition: a cardiovascular MR study with ex-vivo validation. Circ Cardiovasc Imaging 2013; 6:218-28. doi: 10.1161/CIRCIMAGING.112.000133.
4. Kali A, Cokic I, Tang R, et al. Persistent Microvascular Obstruction After Myocardial Infarction Culminates in the Confluence of Ferric Iron Oxide Crystals, Proinflammatory Burden, and Adverse Remodeling. Circ Cardiovasc Imaging 2016;9. pii: e004996.
Figures