2811
A Matrix Completion-Based Reconstruction of In Vivo Eye Images from Undersampled Cartesian 7T MRF Data1Radiology, Leiden University Medical Center, Leiden, Netherlands, 2Ophthalmology, Leiden University Medical Center, Leiden, Netherlands, 3Philips Research Hamburg, Hamburg, Germany
Synopsis
Eye motion is the main challenge in ocular MRF scans. To achieve good MRF image quality on one side and to improve patient comfort on the other side, scan times need to be reduced. In this single-channel coil approach with Cartesian sampling, high undersampling can be supported by using the appropriate reconstruction approach. In this work, a matrix completion-based reconstruction was adopted. Resulting parameter maps are compared to maps obtained after a compressed sensing reconstruction, showing that for matrix completion even much greater undersampling factors result in more accurate parameter maps.
Introduction
In ocular imaging, quantitative T1 and T2 measures have been suggested as measures to discriminate between different classes of eye tumors, with potential to influence therapy1,2. Magnetic Resonance Fingerprinting (MRF) is a recently-introduced method for rapid quantitation of relaxation times3. One of the main challenges in ocular imaging is the repetitive in- and through-plane eye motion4. Shortening the scans would reduce motion-related artifacts, but the single-element eye coil5 which is required to maintain visibility of cued-blink instructions4 excludes the possibility of a reduction in acquisition time via parallel imaging. Furthermore, in Cartesian sampling, used here due to the presence of orbital fat around the eye, undersampling artifacts have a structured nature, which increases the temporal coherence3. In this case, direct matching would often give insufficient accuracy for high undersampling factors. Recently, it was shown that Compressed Sensing (CS) with a total variation regularization constraint in three dimensions helps to improve the quality of the parameter maps for randomly undersampled Cartesian data, but the undersampling factors are still relatively small6. Higher acceleration might be feasible if the correlation in the temporal dimension is better utilized7, such as is the case in matrix completion-based reconstructions8. In this work such a matrix completion-based reconstruction is implemented and results are compared to a CS reconstruction in terms of the quality of the parameter maps.Methods
Experiments were performed on healthy volunteers, with informed consent obtained, using a 7T MR system (Philips Healthcare) equipped with a quadrature head volume coil (Nova Medical) for transmission and a custom-built single-channel eye coil5 for reception.
Fingerprinting definition: A “sinusoidal” pattern of 240 flip angles ranging from 0° to 60° was used preceded by an inversion pulse6. The TE/TR/RF-phase was fixed to 3.5 ms/11 ms/0°. The dictionary was calculated using the extended phase graph formalism7. 165.000 signal evolutions were simulated with T1 and T2 values ranging from 10-6000 ms and 5-500 ms and a B1+ fraction ranging from 0.5-1.0, respectively. A repetition delay of two seconds was chosen10, in which subjects were instructed to blink5.
Data acquisition: Because of the orbital fat around the eye and the sensitivity of spiral acquisitions to off-resonance11, resulting in blurring, Cartesian sampling was used to acquire a fully sampled MRF set with the following scan parameters: FOV 80x80 mm2, resolution 1.0x1.0x6.0 mm3 and scan time of 7:02 minutes. All subjects were instructed to focus on a fixation target during data acquisition.
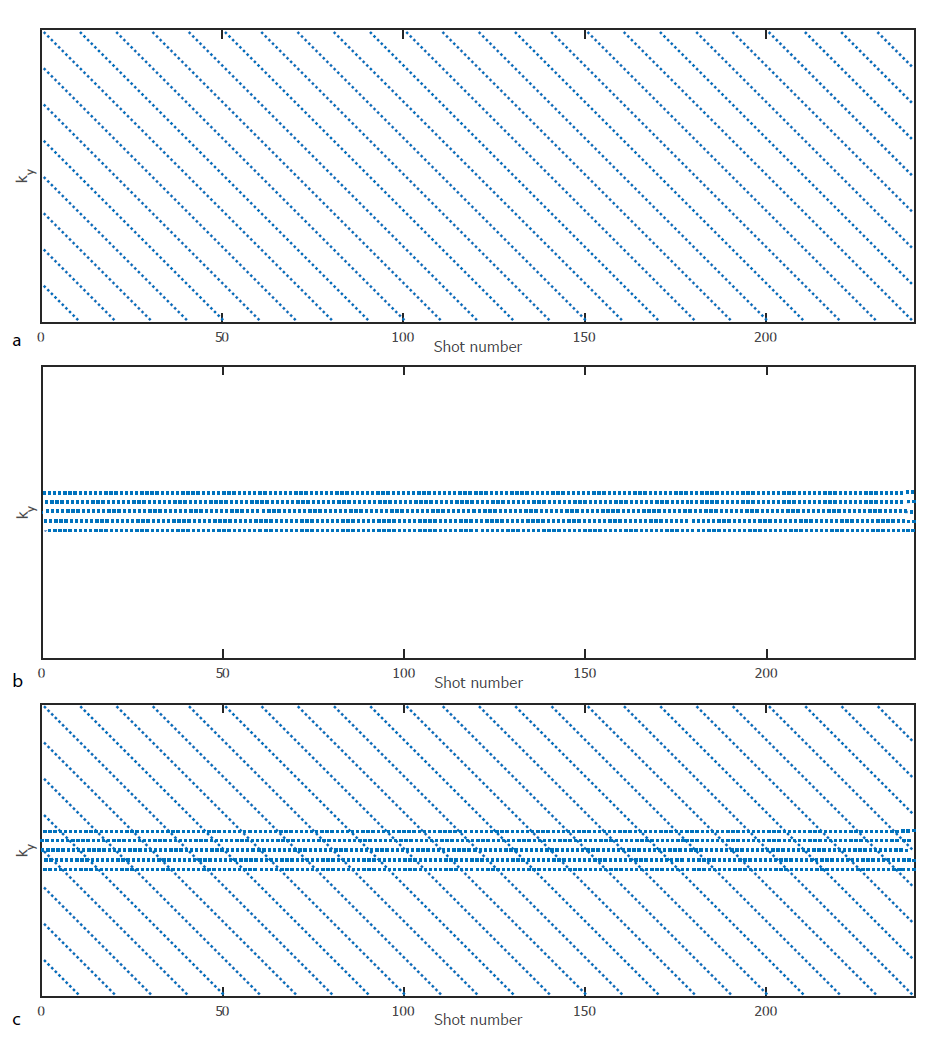
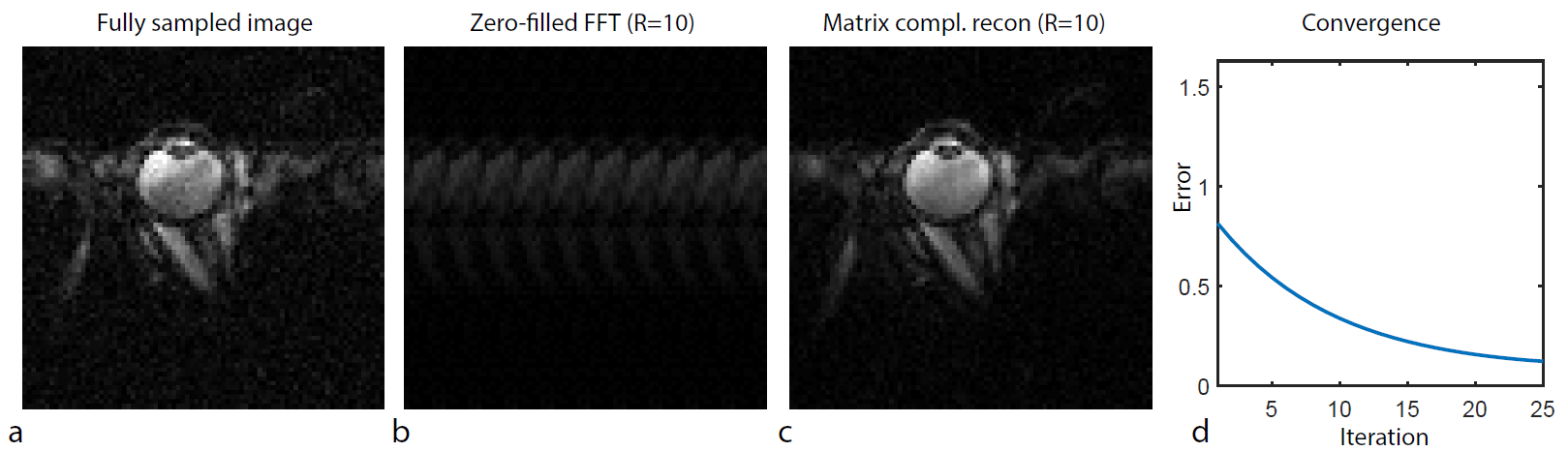
Subsampling and Reconstruction: The fully sampled data set was subsampled using different uniform undersampling line masks for each time frame, such that in each frame the acquired lines are shifted by one $$$ \Delta \text{k}_x $$$ (of the full k-space) with respect to the lines in the previously sampled frame (Fig. 1). A matrix completion-based reconstruction was performed by iteratively solving $$$M = \text{argmin} \lVert \hat{M} \rVert_*$$$ s.t. $$$\mathcal{P}_{\Omega}\hat{M}=M_u$$$ through subspace projection, with $$$\lVert \cdot \rVert_*$$$ the nuclear norm, $$$M_u$$$ the undersampled k-space data, $$$\mathcal{P}_\Omega$$$ the sampling operator and $$$M$$$ the estimate of the true image series8. In this process, 10% of the fully sampled central k-space was used as calibration data from which the 5 most significant singular values were used in the low rank projection of the data. The reconstructed image series for R=10 (plus calibration region) were matched to the dictionary to produce T1, T2, M0 and B1+ maps, and results were compared to a CS approach with R= 4 (details described in ref. 6).
Results
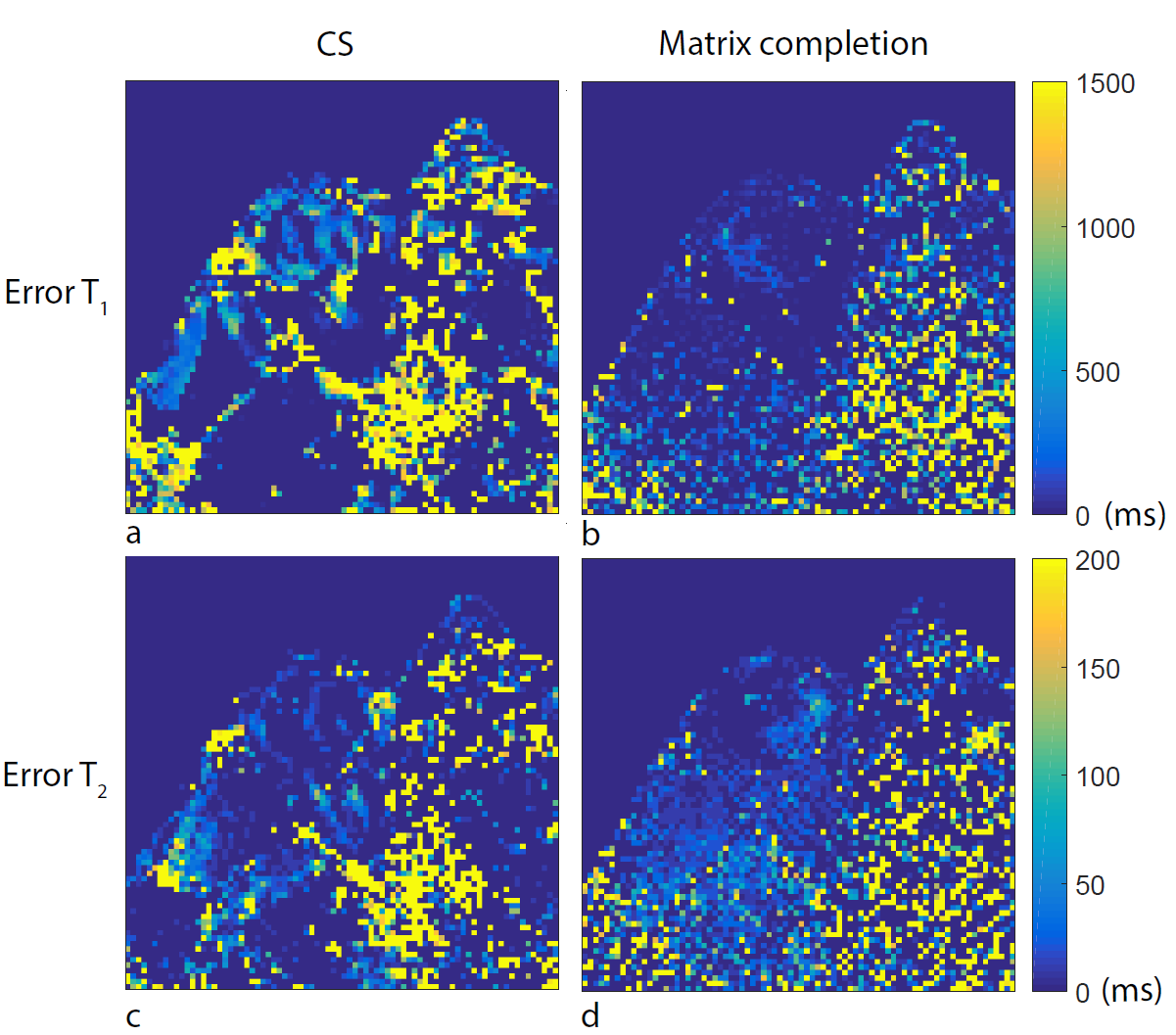
Figure 2 shows the reconstruction results using matrix completion with an undersampling factor of 10. The effect of matrix completion-based reconstruction on the matched parameter maps can be seen in Fig. 3, and maps are compared to the ones obtained from the fully sampled data set and the CS reconstruction. Error maps, defined as the absolute difference map with respect to parameter maps obtained from the fully sampled data set, are shown in Fig. 4. Mean values for the T1/T2 of the vitreous body, the fat and the eye lens are 3840/145 ms, 71/59 ms and 1250/25 ms, respectively, which agree with values published in previous literature12.Discussion
The results in this study show the benefit of utilizing the temporal dimension in the reconstruction of MRF data, as exemplified by matrix completion. The low rank property of the signal evolutions allows one to reach higher undersampling factors than in a CS reconstruction, which mainly exploits sparsity in the spatial domain. In ocular imaging, these high undersampling factors can be used to shorten scan time and in that way reduce motion artifacts, which is particularly important for elderly patients, who typically experience difficulties focusing on a fixation target.Acknowledgements
This project was funded by the European Research Council Advanced Grant 670629 NOMA MRI.References
- Chambers R et al. Magnetic Resonance Imaging of Uveal Melanomas. Archives of Ophthalmology. 1987;105:917-921.
- Rofstad E et al. Magnetic Resonance Imaging of Human Melanoma Xenografts in Vivo: Proton Spin–lattice and Spin-spin Relaxation Times Versus Fractional Tumour Water Content and Fraction of Necrotic Tumour Tissue. International Journal of Radiation Biology. 1994;65(3):687-401.
- Ma D et al. Magnetic Resonance Fingerprinting. Nature. 2013;495:187-192.
- Berkowitz B et al. Measuring the Human Retinal Oxygenation Response to a Hyperoxic Challenge Using MRI: Eliminating Blinking Artifacts and Demonstrating Proof of Concept. Magnetic Resonance in Medicine. 2001;46:412-416.
- Beenakker J et al. Clinical evaluation of ultra-high-field MRI for three-dimensional visualisation of tumour size in uveal melanoma patients, with direct relevance to treatment planning. Magnetic Resonance Materials in Physics, Biology and Medecine. 2016;29:571-577.
- Koolstra K et al. The Effect of Compressed Sensing on the Quality of Cartesian MRF Parameter Mapping in the Eye at 7T. Workshop on Magnetic Resonance Fingerprinting. 2017:15.
- Tsao J et al. k-t BLAST and k-t SENSE: Dynamic MRI With High Frame Rate Exploiting Spatiotemporal Correlations. Magnetic Resonance in Medicine. 2003;50:1031-1042.
- Doneva M et al. Matrix completion-based reconstruction for undersampled magnetic fingerprinting data. Magnetic Resonance Imaging. 2017;41:41-52.
- Scheffler K. A Pictorial Description of Steady States in Rapid Magnetic Resonance Imaging. Concepts in Magnetic Resonance. 1999;11:291-304.
- Amthor T et al. Magnetic Resonance Fingerprinting with short relaxation intervals. Magnetic Resonance Imaging. 2017;41:22-28.
- Börnert P et al. Improvements in spiral MR imaging. Magnetic Resonance Materials in Physics, Biology and Medicine. 1999;9:29-41.
- Richdale K et al. 7T MR Imaging of the Human Eye In Vivo. Journal of Magnetic Resonance Imaging. 2009;30(5):924-932.
Figures