2686
Reformattable MAVRIC-SL Using Robust Principal Component Analysis and Variable Density Complementary Poisson Disc Sampling1Electrical Engineering, Stanford University, Stanford, CA, United States, 2Radiology, Stanford University, Stanford, CA, United States
Synopsis
MAVRIC-SL resolves metal-induced artifacts at the cost of additional scan time. A reconstruction using Robust Principal Component Analysis (RPCA) has been shown to considerably reduce scan times with minimal loss in image quality. We apply this scan time reduction to acquire isotropic MAVRIC-SL data that can be reformatted to all three planes, combining multiple high-resolution scans into a single, short, isotropic scan. We show retrospectively undersampled isotropic MAVRIC-SL RPCA reconstructions reformatted to three planes for the case of a hip phantom, and a volunteer with a titanium hip replacement. The RPCA reconstruction offers good image quality in multiple planes at clinically feasible scan times, with shorter scan times than separate high-resolution acquisitions.
Introduction
MAVRIC-SL1 is a 3D multispectral sequence that resolves imaging artifacts near metal by acquiring the volume with different spectral weightings, creating a fourth dimension referred to as bins. While reducing metal-induced artifacts, MAVRIC-SL suffers from increased scan times due to the acquisition of the additional bin dimension. A recently introduced reconstruction technique2 applied Robust Principal Component Analysis (RPCA)3 and variable density complementary Poisson disc4 (VDCPD) sampling in the ky-kz plane to substantially reduce MAVRIC-SL scan times with minimal loss in image quality.
In this work, we apply this scan time reduction to demonstrate high-resolution Multi-Planar Reformatting (MPR) MAVRIC-SL with retrospective scan times of less than 7 minutes with 1.6 mm isotropic voxels. The purpose is to replace two or three scans with different imaging planes with a single isotropic scan that can be acquired at overall reduced scan times and be reformatted to all three planes. We present retrospective undersampled scan times that could be acquired using MPR MAVRIC-SL, and demonstrate clinically feasible scan times at comparable image quality in two scan planes.
Methods
To demonstrate the utility of MPR MAVRIC-SL, we acquired a reference isotropic dataset of a titanium hip phantom submerged in agar, and a volunteer with a titanium hip replacement in the left hip. We performed retrospective undersampling using both VDCPD and uniform undersampling and compared the RPCA reconstruction to conventional parallel imaging.
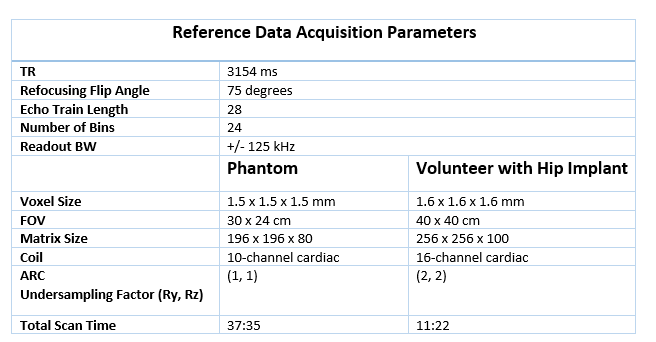
All images were acquired coronally on GE 3T MRI systems using a proton-density weighted MAVRIC-SL acquisition. For the in-vivo scan, the volunteer signed an informed consent form approved by the institutional review board. Scan parameters used to acquire the reference data are summarized in Figure 1. Each of these scans were reconstructed using autocalibrating parallel imaging (ARC)5 to form a reference data set. The reference isotropic acquisitions were retrospectively undersampled in the ky-kz plane and reconstructed at different undersampling factors using equation (12) from Levine et al.2, with coil compression to n=10 coils6, virtual conjugate coils7, and calibration-free locally low–rank encouraging reconstruction (CLEAR)8. Reconstruction parameters were $$$\lambda_S=0.005,\lambda_C=0.0003$$$, identity sparsity transform, 50 iterations. The phantom RPCA reconstruction was compared to retrospective uniform undersampling reconstructions using ARC, with a 16 x 16 ky-kz calibration region and a 9 x 9 kernel.
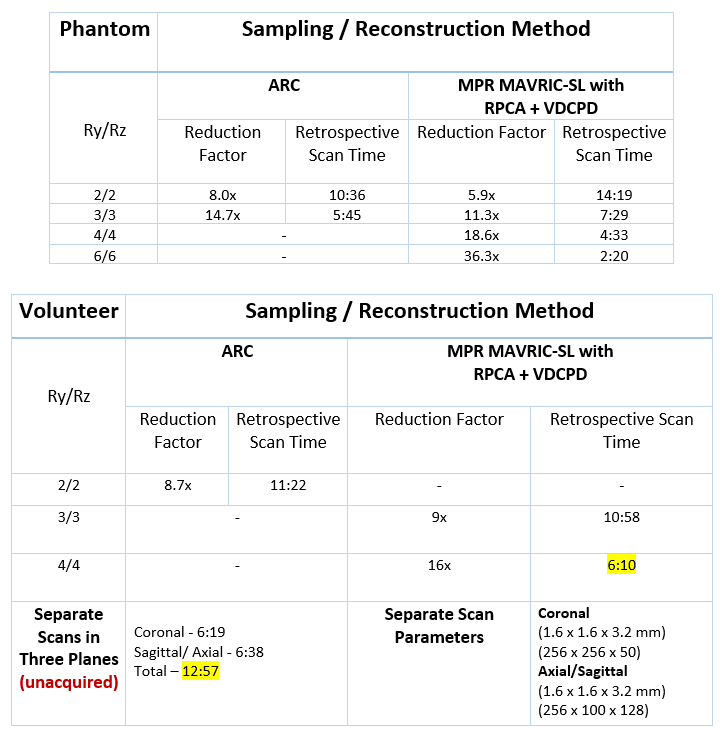
Retrospective acquisition times were estimated by counting ky-kz phase encode lines after retrospective undersampling and dividing by the number of ky-kz phase encode lines in the reference acquisition. Reduction factors listed for each undersampling technique are relative to fully sampled Cartesian ky-kz k-space with no corner cutting or partial Fourier.
We compared RPCA+VDCPD retrospective scan times to scan times for separate high-resolution acquisitions of the coronal view and axial/sagittal (unacquired). The matrix sizes for separate scans were determined by assuming an isotropic acquisition at 1.6 mm and a full matrix size of 256 x 256 x 100.
Results
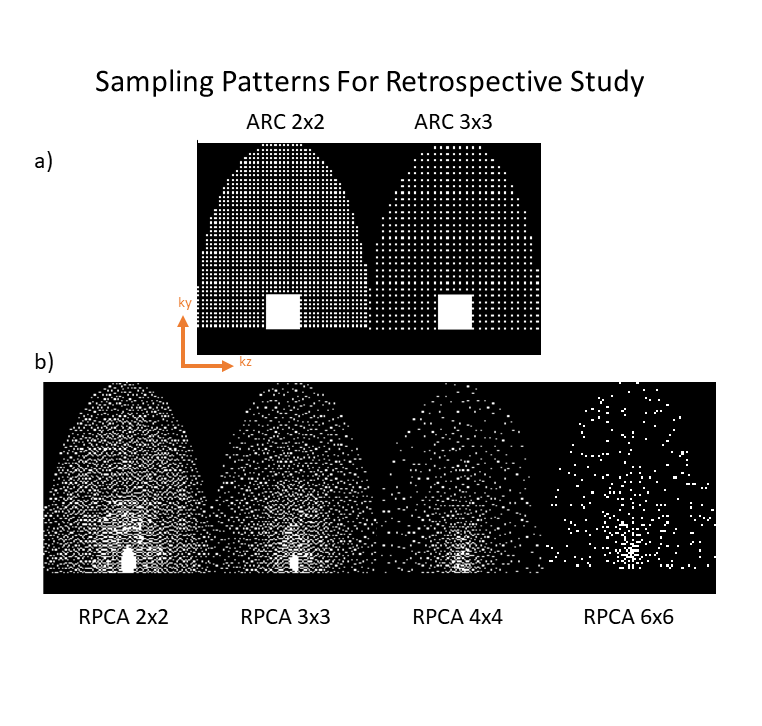
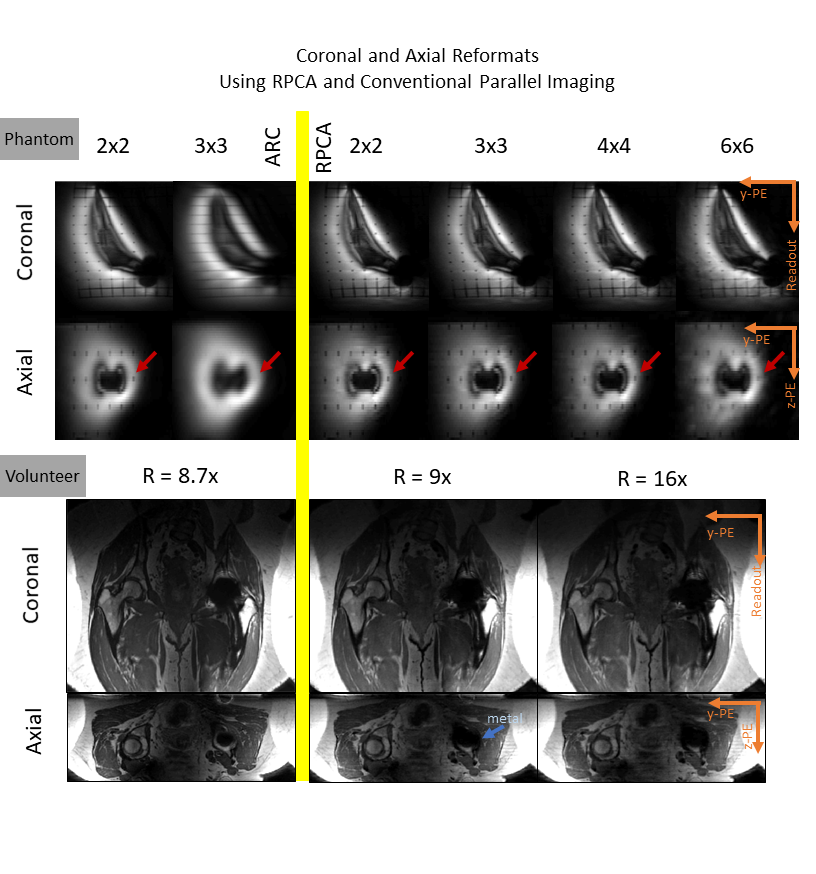
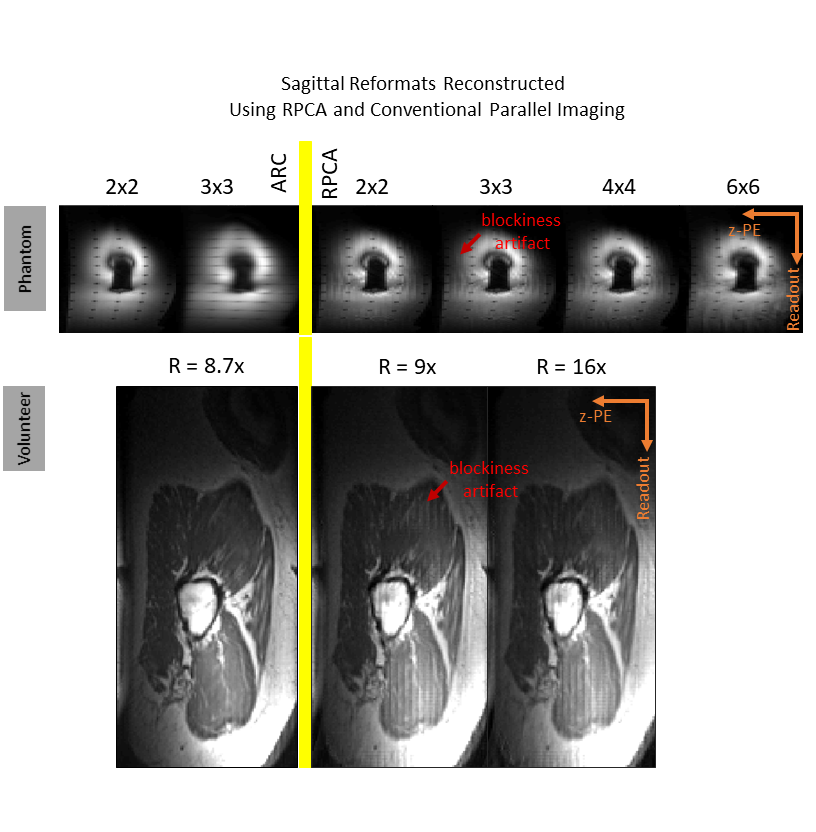
Sampling patterns for the retrospective reconstructions are shown in Figure 2. The estimated acquisition times and reduction factors over fully sampled cartesian using the studied sampling patterns are shown in Figure 3. Coronal and axial images reconstructed using the RPCA and ARC methods are shown in Figure 4. These images have comparable image quality to the reference dataset. Reformatted sagittal views are shown in Figure 5, and have a "blockiness" artifact sometimes observed in compressed sensing.Discussion
The RPCA reconstruction at high undersampling factors maintains good image quality in the coronal and axial planes while the ARC reconstruction has dramatic resolution loss at Ry=3, Rz=3 shown in Figure 4. At Ry=3, Rz=3, the retrospective acquisition time using RPCA reconstruction is equivalent to two separate high-resolution scans. At R=16x, the retrospective acquisition time using RPCA reconstruction is clinically feasible. Beyond Ry=4, Rz=4, the phantom RPCA reconstruction has noticeable blurring due to increased undersampling of outer k-space and residual reconstruction artifacts.
The sagittal reformats with the fully sampled readout and undersampled ky direction are of poor diagnostic quality and we are currently working to address the blockiness artifact in this reformat plane. However, simultaneously acquiring coronal and axial views still has superior scan times to two separate acquisitions as shown in Figure 3. The tradeoff of the isotropic acquisition's improved scan time is a small SNR penalty due to reduced voxel size, which can be offset by averaging in the slice direction of the reformatted view plane.
Conclusion
We have demonstrated that MPR MAVRIC-SL can be achieved in clinically feasible scan times using VDCPD sampling and RPCA reconstruction, combining multiple high-resolution scans into one reformattable isotropic scan.Acknowledgements
R01 EB017739. GE Healthcare.References
- Koch K, et al. Imaging near metal with a MAVRIC-SEMAC hybrid. MRM. 2007;65(1):71-82.
- Levine E, et al. Accelerated three-dimensional multispectral MRI with robust principal component analysis for separation of on- and off-resonance signals. MRM. 2017. DOI: 10.1002/mrm.26819.
- Candes E, et al. Robust Principal Component Analysis? Journal of the ACM. 2008;346(9-10):589-592.
- Levine E, et al. 3D cartesian MRI with compressed sensing and variable view sharing using complementary poisson-disc sampling. MRM. 2016.
- Brau A, et al. Comparison of reconstruction accuracy and efficiency among autocalibrating data-driven parallel imaging methods. MRM. 2008;59:382-395.
- Zhang T, et al. Coil compression for accelerated imaging with cartesian sampling. MRM. 2013;69(2):571-582.
- Blaimer M, et al. Virtual coil concept for improved parallel MRI employing conjugate symmetric signals. MRM. 2009;61(1);93-102.
- Trzasko J, et al. Calibrationless parallel MRI using CLEAR. Signals, Systems and Computers (ASILOMAR), 2011 Conference Record of the Forty Fifth Asilomar Conference on, pages 75-79. 2011.
Figures