2685
Rotating Outer Volume Suppression for Reduced Field of View PROPELLER Imaging1Global MR Applications & Workflow, GE Healthcare, New York, NY, United States, 2Global MR Applications & Workflow, GE Healthcare, Menlo Park, CA, United States, 3GE Healthcare, Haifa, Israel, 4GE Healthcare, Waukesha, WI, United States, 5Global MR Applications & Workflow, GE Healthcare, Houston, TX, United States
Synopsis
We present a modified PROPELLER pulse sequence that incorporates rotating outer volume suppression for reduced field of view imaging. In vivo results are presented, demonstrating comparable imaging performance with conventional PROPELLER imaging.
Introduction
Efficient, motion-robust imaging remains a challenge and a critical need in clinical MR imaging. PROPELLER (aka BLADE, MultiVane etc.) is a two-dimensional imaging technique that leverages redundancies in the acquired data to retrospectively correct for in-plane motion and to mitigate the effects of through-plane motion [1]. PROPELLER's inherent motion robustness comes at the cost of longer imaging times (versus Cartesian equivalents), due to redundant sampling near the center of k-space, and oversampling in both the frequency and phase directions required to eliminate phase wrap. The latter no-wrap penalty also tends to limit the minimum useable FOV due to practical constraints on scan time. Outer volume suppression (OVS) has been shown to be useful in the context of 2D and 3D echo-train imaging for reducing scan time and for improving image quality [2-5]. Here, we introduce OVS for PROPELLER imaging and consider its utility.Materials & Methods
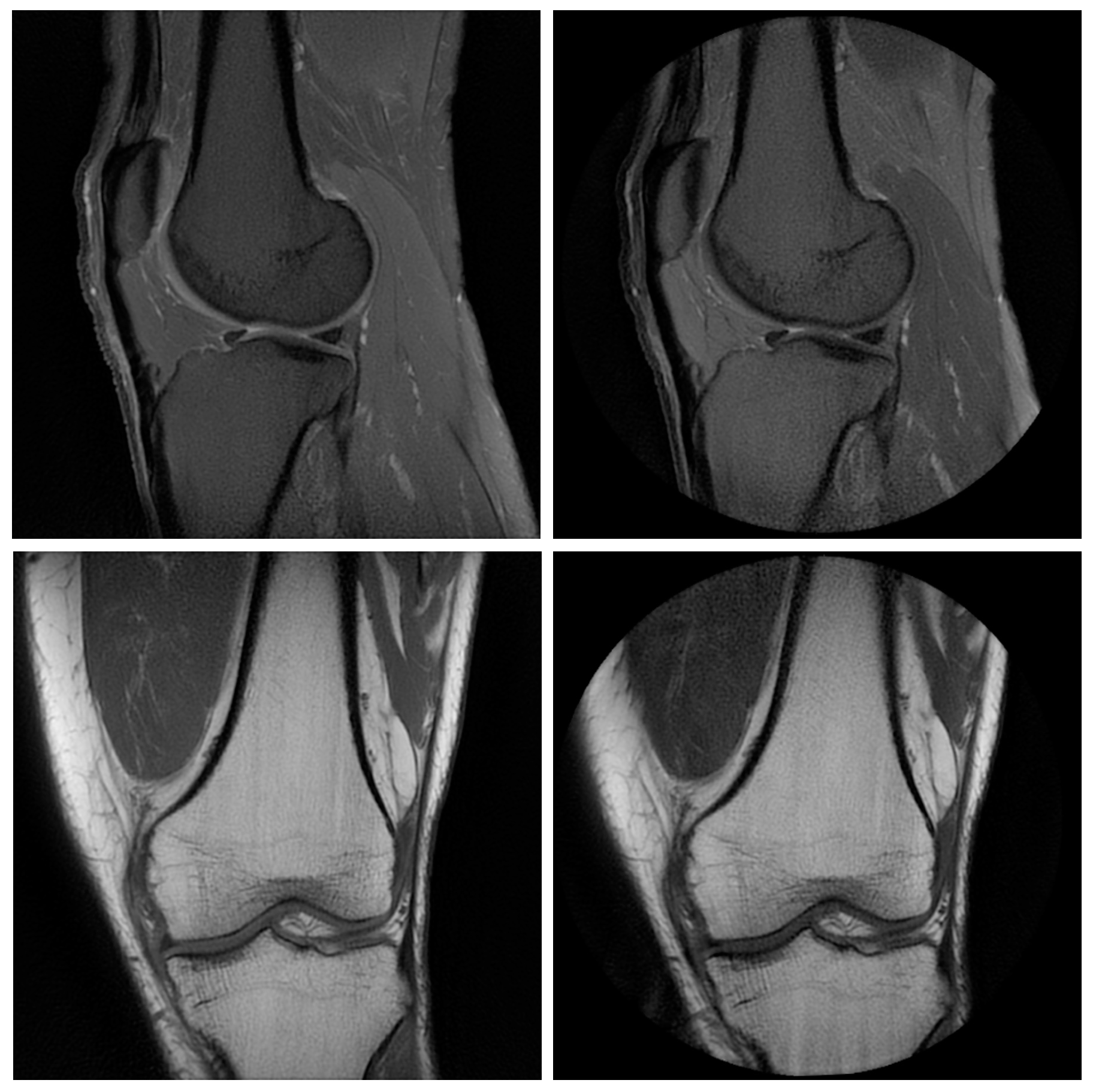
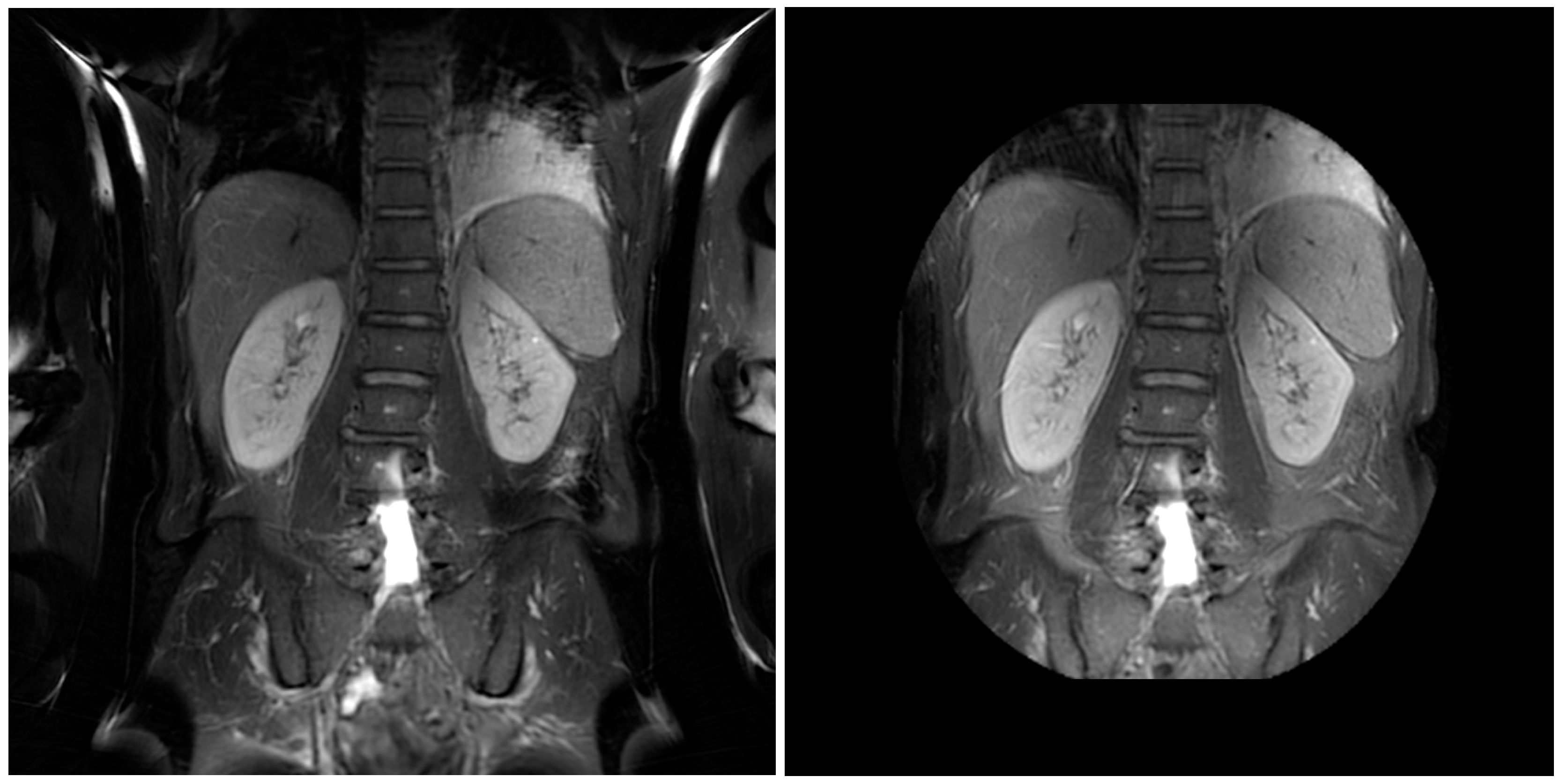
A conventional PROPELLER pulse sequence was modified to incorporate a set of very-selective saturation (VSS) pulses [2,3]. In the modified acquisition, VSS bands are applied symmetrically in the phase-encoded direction of each PROPELLER blade. These saturation bands are rotated incrementally along with the blade throughout the course of the acquisition to provide rotationally-symmetric OVS. This enables PROPELLER imaging with reduced oversampling requirements, allowing for faster imaging and/or reduced fields-of-view. Following informed consent, several volunteers were scanned under IRB approval on a 60-cm 3.0T MRI scanner (Discovery MR750, GE Healthcare, Waukesha, WI) and 70-cm 1.5T MRI scanner (Optima MR450w, GE Healthcare, Waukesha, WI). A variety of anatomies and scan planes were imaged with PROPELLER using conventional oversampling and rotating OVS. The number of VSS pulses applied per echo train ranged from 1 to 3, and other imaging parameters are summarized in Table 1.Results & Discussion
PROPELLER imaging results for pelvis, knee, and abdomen are summarized in Figures 1 through 4. As indicated in Table 1, reductions in scan time ranged from 9% to 31% at 1.5T and from 7% to 26% at 3T. Similar contrast and image quality is observed in both the conventional, oversampled and reduced-FOV PROPELLER acquisitions at the expense of a modest and expected reduction in SNR.
These promising early results demonstrate the feasibility of using rotating VSS pulses to perform rotationally symmetric OVS for PROPELLER without oversampling in the phase or frequency direction. The introduction of OVS eliminates PROPELLER’s phase-wrap oversampling penalty, but necessarily increases the repetition time (TR) due to increased radiofrequency (RF) power deposition from the VSS pulses. The impact of heating is especially notable at 3T, and therefore, reductions in scan time are not directly proportional to the reduction in oversampling, and less so for shorter echo train lengths, as in T1-weighted imaging. The challenge of optimizing this OVS technique, therefore, is largely one of managing RF power and mitigating SNR impacts.
A full exploration of the tradeoffs between and technical optimization of the OVS implementation is beyond the scope of this early work, but due to its pseudo-radial design, PROPELLER is inherently robust to aliasing artifacts (versus conventional Cartesian FSE, for example) suggesting that it may require less intensive or less frequent application of VSS pulses and that further reductions in scan time might be achieved without loss of OVS performance.
Conclusions
We have demonstrated the feasibility of using rotating VSS bands for faster and more flexible PROPELLER imaging. PROPELLER images free from oversampling in the phase and frequency directions were demonstrated in vivo with comparable image quality to those generated with conventional PROPELLER acquisitions. OVS performance must be balanced against SAR and SNR considerations, and a complete analysis of robustness, contrast, and clinical performance is left for future work.Acknowledgements
No acknowledgement found.References
- Pipe JG. Motion correction with PROPELLER MRI: application to head motion and free-breathing cardiac imaging. Magn Reson Med. 1999 Nov;42(5):963-9.
- Le Roux P, Gilles RJ, McKinnon GC, Carlier PG. Optimized outer volume suppression for single-shot fast spin-echo cardiac imaging. J Magn Reson Imaging. 1998 Sep-Oct;8(5):1022-32.
- Osorio JA, Xu D, Cunningham CH, Chen A, Kerr AB, Pauly JM, Vigneron DB, Nelson SJ. Design of cosine modulated very selective suppression pulses for MR spectroscopic imaging at 3T. Magn Reson Med. 2009 Mar;61(3):533-40.
- Banerjee S, Han M, Chen W, Hess CP, Krug R, Shankaranarayanan A, Zur Y. Reduced field-of-view imaging with 3D variable flip angle Fast Spin Echo-feasibility in MRI of orbits. Proc. Intl. Soc. Mag. Reson. Med. 23 (2015).
- Taviani V, Litwiller D, Loening AM, Saranathan M, Hargreaves BA, Vasanawala SS. Single-Shot Fast Spin Echo of Targeted Regions with Variable Refocusing Flip Angles and Quadratic Phase Pulses for Outer Volume Suppression. Proc. Intl. Soc. Mag. Reson. Med. 23 (2015).
Figures