2675
A Two-Dimensional Spiral Multi-Echo Turbo-Spin-Echo Technique1Barrow Neurological Institute, Phoenix, AZ, United States, 2Philips Healthcare, Cleveland, OH, United States
Synopsis
TSE is widely used for T2 weighted imaging in routine clinical neuro exams. However, the concerns with TSE include its high specific absorption rate (SAR), and difference in contrast compared to conventional SE. In this work we propose a 2D spiral multi-echo TSE technique, which is insensitive to the T2-decay induced signal variation that affects other spiral TSE techniques. This technique provides improved contrast, high signal to noise ratio, and substantially reduced SAR, compared to Cartesian TSE.
Introduction
T2-weighted (T2w) imaging is commonly used in routine clinical exams, especially for neuroimaging. Conventional spin-echo (SE) has been replaced by rapid acquisition with relaxation enhancement (RARE, or fast/turbo-spin-echo, FSE/TSE) for T2w imaging due to its high speed (1). However, a major concern with TSE is its high specific absorption rate (SAR) associated with the long radio frequency (RF) pulse train, especially at high field strengths (2). In addition, the use of a long RF pulse train may alter the T2 contrast (3).
Various investigations have been conducted to reduce the SAR and improve the contrast. A spiral SE technique has been proposed to provide fast speed and superior T2 contrast, but the signal-to-noise ratio (SNR) is suboptimal (4). Incorporating the spiral trajectory in 2D TSE can provide fast speed and low SAR. However, T2-decay induced signal modulation in k-space, if not corrected, can lead to swirl-like artifacts. A spiral-ring TSE technique has been implemented without these artifacts, but may be prone to blurring and off-resonance related artifacts (5). Recently a spiral TSE sequence with a double encoding and signal demodulation strategy has been shown to produce high SNR and improved contrast, with the swirl-like artifacts effectively minimized (6). Nonetheless, the signal demodulation may have different impact on normal tissues and lesions. In addition, the contrast has contributions from both early and late echoes, since all spiral interleaves traverse the center of k-space. Therefore, further clinical validation is required.
To avoid these concerns, we propose a spiral multi-echo TSE (spiral mTSE) technique, which is insensitive to the T2-decay induced signal variation, and also improves the contrast.
Methods
With the spiral mTSE technique, multi-echo data are acquired, and separate images are reconstructed for each echo (e.g, S1 to S5, with an ETL = 5). Since the data for a single echo are not affected by the T2-decay induced signal variation, these individual images are not contaminated by the aforementioned artifacts, so is the final image generated by combining these individual images. Secondly, rather than using an arithmetic mean which may not generate optimal contrast, the individual images are combined using a modified geometric mean:
$$\begin{aligned}I &= (\sqrt{S1\times S5}+\sqrt{S2\times S4}+S3) / 3 \\&= (\sqrt{S0\cdot e^{-TE1/T2} \times S0\cdot e^{-TE5/T2}}+\sqrt{S0\cdot e^{-TE2/T2} \times S0\cdot e^{-TE4/T2}}+S0\cdot e^{-TE3/T2})/3 \\&= (S0\cdot \sqrt{e^{-(TE1+TE5)/T2}}+S0\cdot \sqrt{e^{-(TE2+TE4)/T2}}+S0 \cdot e^{-TE3/T2})/3 \\&= (S0\cdot e^{-TE3/T2}+S0\cdot e^{-TE3/T2}+S0\cdot e^{-TE3/T2})/3 \\&=S0\cdot e^{-TE3/T2}\end{aligned}$$
where S0 is the spin density. This produces a T2 contrast reflecting the true TE (i.e., TE3), unlike the arithmetic mean. Instead of a simple geometric mean over all five echoes, the modified geometric mean is adopted to improve the noise performance.
Acquiring fully sampled data for each echo requires a longer scan time compared to spiral TSE. Undersampled variable density data are collected with a reduction factor of 2.5 to reduce the scan time to a level comparable to that of spiral TSE, and reconstructed using iterative SENSE (7).
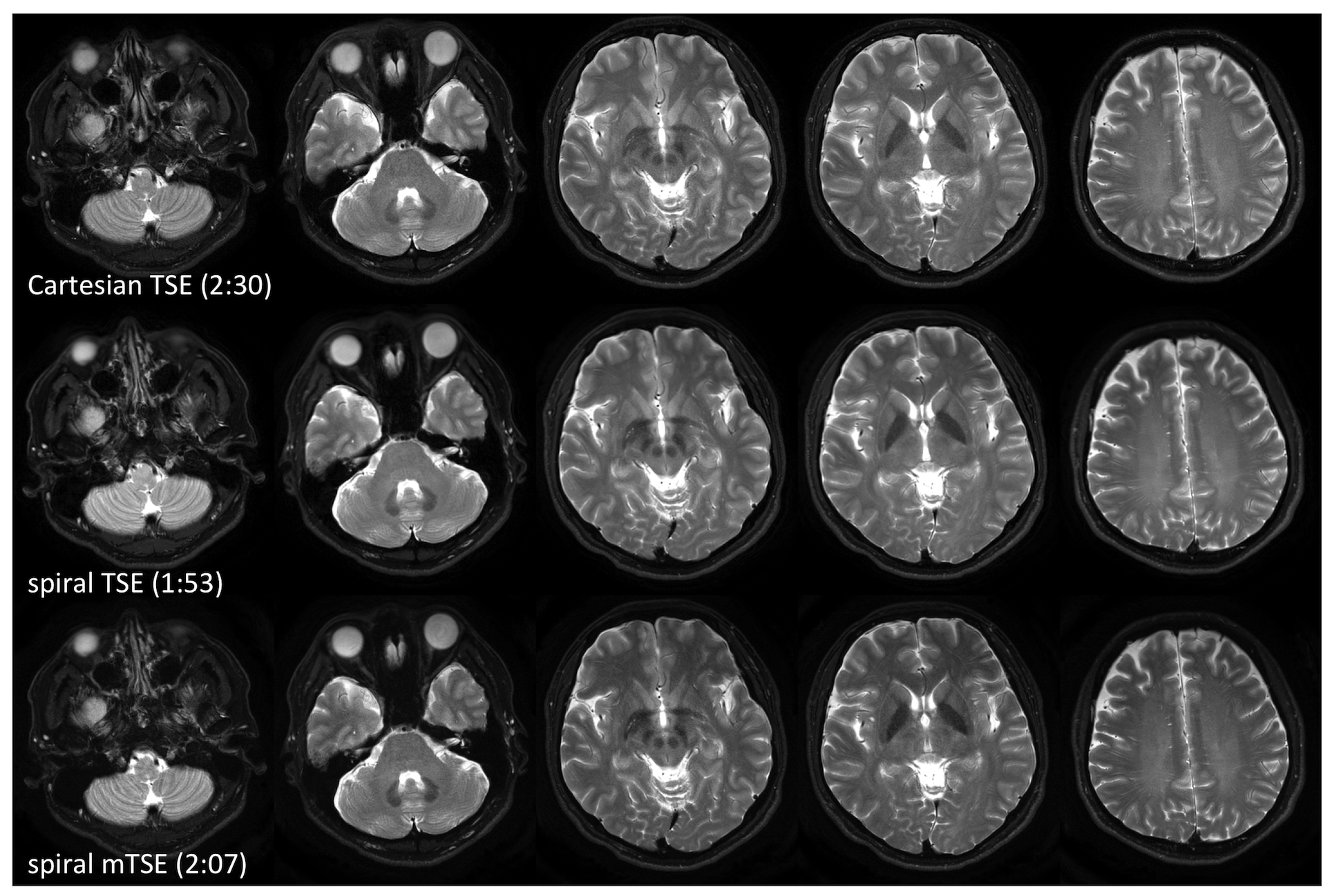
The spiral mTSE sequence was implemented on a 3T Philips Ingenia scanner. Volunteer data were acquired after approval from the institutional review board. Data were also acquired with Cartesian TSE and spiral TSE for comparison. The scan time is 2:07, 1:53, and 2:30, for spiral mTSE, spiral TSE, and Cartesian TSE, respectively.
Results and Discussion:
Fig. 1 shows the images acquired with Cartesian TSE, spiral TSE, and spiral mTSE. There are no visible swirl-like artifacts in the spiral mTSE images that can be attributed to the T2-decay induced signal variation, indicating that the proposed multi-echo strategy is effective.
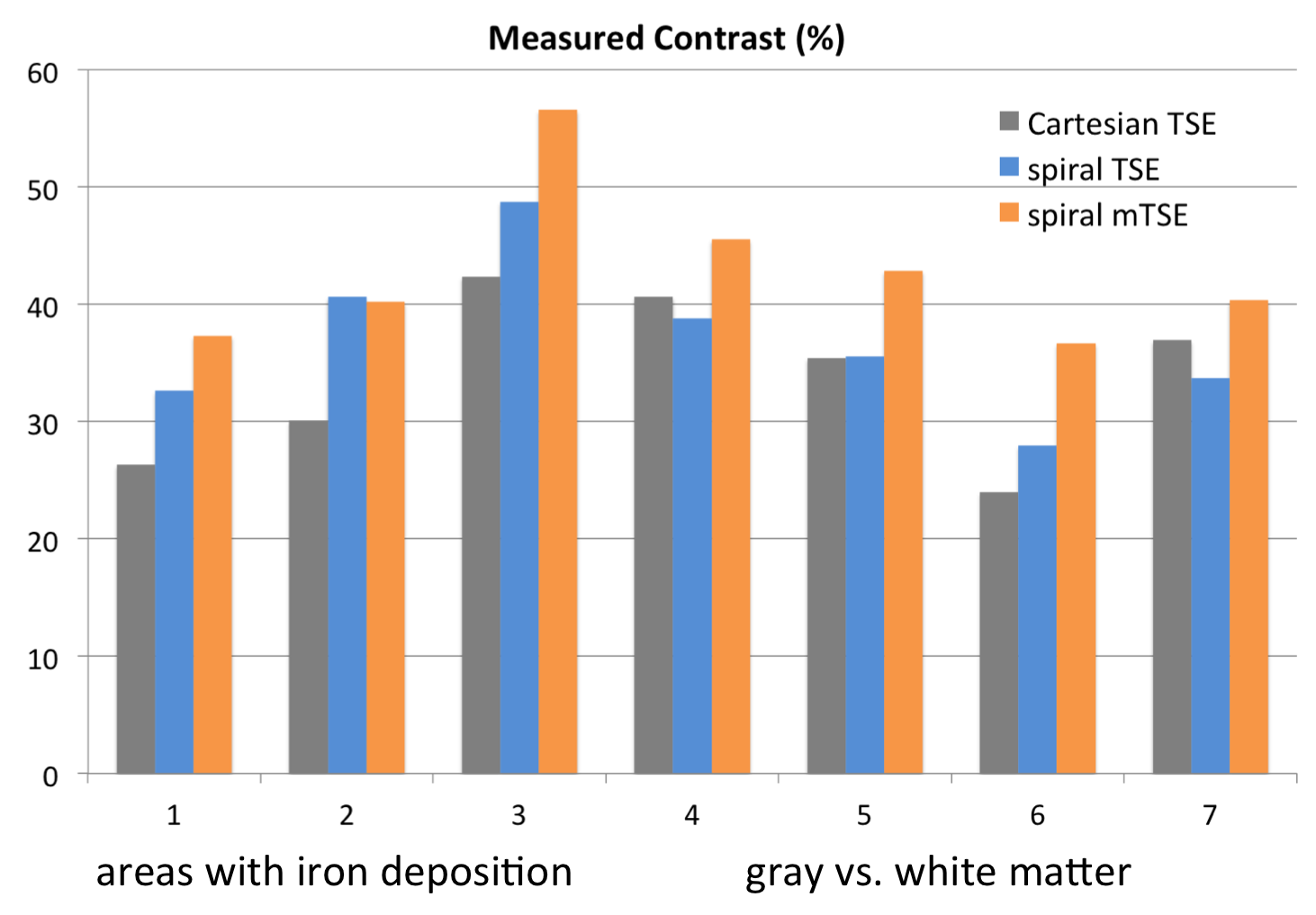
As can be seen with the images as well as from the measured contrast shown in Fig. 2, spiral TSE exhibits comparable white-to-gray matter contrast while improving the contrast in areas with iron deposition, compared to Cartesian TSE. With the proposed spiral mTSE technique, further improvement is evident for both white-to-gray matter contrast and contrast in gray matter nuclei with iron deposition. Visual inspection indicates that the SNR of spiral mTSE is superior to Cartesian TSE, although it is slightly lower than spiral TSE, primarily due to the g-factor from parallel imaging and the non-linear combination of the individual images.
In addition, like spiral TSE, spiral mTSE has inherently low SAR due to the short echo train (5, vs 19 in Cartesian TSE), allowing a higher refocusing flip angle (180°, vs 120° in Cartesian TSE).
Conclusion:
The proposed spiral mTSE is insensitive to the T2-decay induced signal variation, improves contrast, and produces high SNR and low SAR. Therefore, it provides a promising alternative to conventional TSE for rapid T2w neuroimaging. Upcoming clinical trials will compare the clinical efficacy of spiral TSE and mTSE vs. standard Cartesian TSE.Acknowledgements
This work was funded by Philips Healthcare.References
(1). Hennig J, Nauerth A, Friedburg H. RARE Imaging: A Fast Imaging Method for Clinical MR. Magn Reson Med. 1986;3:823-833.
(2) Hennig J. Multiecho Imaging Sequences with Low Refocusing Flip Angles. J Magn Reson. 1988;79:397-407.
(3) Constable RT, Anderson AW, Zhong J, et al. Factors Influencing Contrast in Fast Spin-Echo MR Imaging. Magn Reson Imaging. 1992;10:497-511.
(4) Li Z, Wang D, Karis JP, Pipe JG. A Spiral Spin-Echo Sequence for Fast T2-Weighted Imaging with Improved Contrast. ISMRM 2015;23:p2444.
(5) Block W, Pauly J, Nishimura D. RARE spiral T2-weighted imaging. Magn Reson Med 1997;37:582–590.
(6) Li Z, Wang D, Robison RK, Karis JP, Pipe JG. A Two-Dimensional Spiral Turbo-Spin-Echo Technique with T2-Decay Correction and Concomitant Phase Compensation. ISMRM 2017;25:p4020.
(7) Pruessmann KP, Weiger M, Bornert P, Boesiger P. Advances in Sensitivity Encoding With Arbitrary k-Space Trajectories. Magn Reson Med. 2001;46:638-651.
Figures