2636
Patient Acceptance on a Compact 3T is Generally Superior to a Whole-Body Scanner1Radiology, Mayo Clinic, Rochester, MN, United States, 2GE Global Reserach, Niskayuna, NY, United States
Synopsis
A compact 3T scanner was developed under a Bioengineering Research Partnership as a technology demonstrator. To assess patient acceptance on the compact 3T compared with a whole-body 3T MR, 33 consecutive patients completed a series of survey questions to report their subjective experience. The survey results demonstrate that the Compact 3T is equal or superior to a whole-body scanner for patient acceptance.
Introduction
One of the most important aspects of MR imaging is to ensure patient comfort during the examination, which improves image quality by reducing patient motion and resulting in an overall positive experience for the patient. Recently a compact 3T1, 2 (C3T) scanner was developed under an NIH-funded Bioengineering Research Partnership between GE Global Research Center and Mayo Clinic, and was installed at Mayo Clinic in February 2016. Due to its reduced bore size (37-cm inner diameter for the head, 60-cm inner diameter for the shoulders); the C3T scanner uses an asymmetric design for the transverse gradient axes to allow patient access. The objective of this study was to evaluate the patient experience on the C3T compared to 60-cm whole-body, commercially-available systems.
Methods
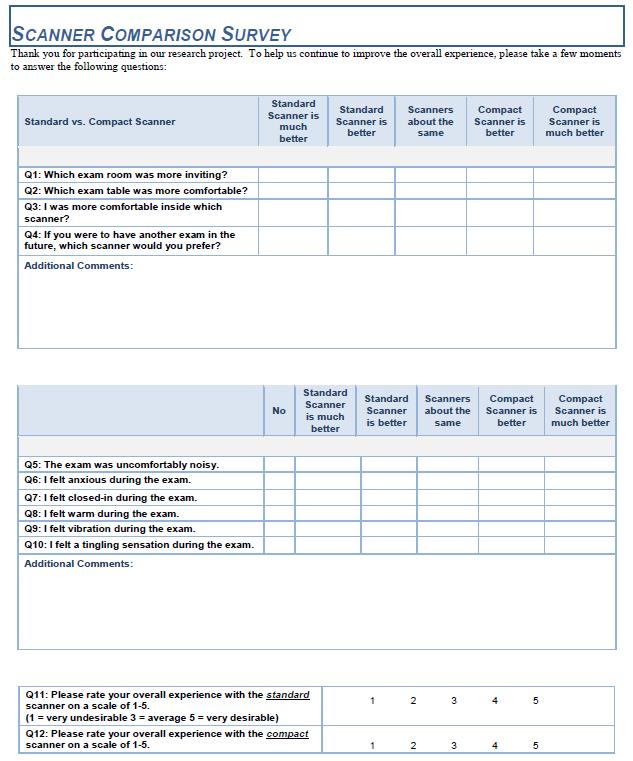
During a prospective imaging study3 comparing the image quality of the C3T scanner and a whole-body 3T scanner, 33 patients (29 brain exams, 4 wrist exams) were asked to complete a survey composed of 12 questions (Fig. 1). Under an IRB-approved protocol, patients were imaged on the C3T scanner, with high performance gradients (80 mT/m, 700 T/m/s)4, and commercially available, whole-body systems (GE MR750 or GE HDx 60-cm bore, 3T, 33-50 mT/m, 150-200 T/m/s). Immediately upon conclusion of the last imaging study, the subjects were asked to complete a questionnaire evaluating the experience on a 5 point scale (1 = standard scanner is much better, 5 = compact scanner is much better, 0 = not applicable). The responses were graded utilizing Wilcoxon signed-rank test. The N/A responses (i.e., 0) were not included in the statistical analysis. For example, a response of “0” on question 6 indicated that the subject did not feel anxious on either scanner.
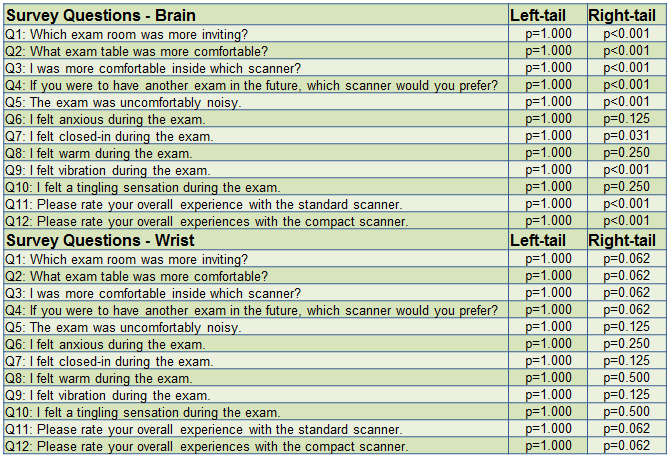
The null hypothesis of the right-tailed test was that the C3T was inferior to a standard, whole-body scanner and the left-sided test used the converse of this hypothesis (Fig 2).
Results
Presuming a 5% significance level, the right-sided test results indicate that the C3T brain exams rated higher than the whole-body system in the following categories: comfort, future exam preference, anxiety and tingling (e.g., caused by PNS). Overall, the C3T was superior or equivalent to a whole-body system (Fig. 3).
One subject reported peripheral nerve stimulation (PNS) at the nasion on the C3T. That issue was subsequently addressed by a minor pulse sequence modification, which did not result in any scan time penalty or image quality compromise, and demonstrated equivalent contrast and lesion conspicuity while completely eliminating the PNS sensation.
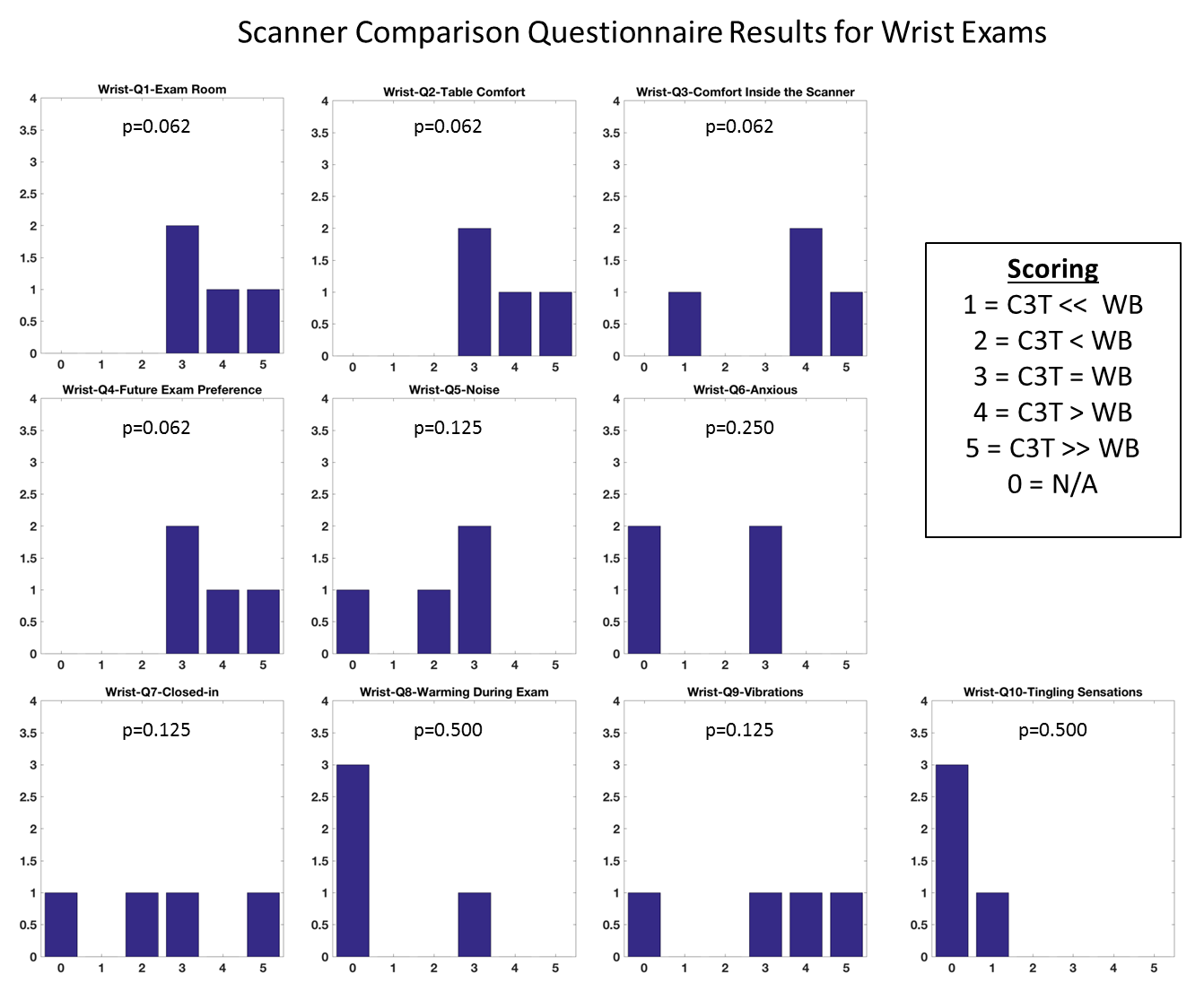
Wrist exams acquired on the C3T demonstrated a higher acceptance level than a whole-body scanner in all 10 direct comparison categories utilizing a right-tailed test and a 5% significance level. Failure of both the left and right-tailed tests to reject the null hypothesis indicate that, for this limited pool of patients, the C3T performed equivalently to the whole-body system (Fig. 4).
Results were also pooled across question utilizing Fisher’s combination, allowing strong rejection of the null hypothesis that the whole-body system was superior to the C3T in terms of patient acceptance, and strong acceptance of the converse.
Discussion
The overall high-degree of patient acceptance reported on the C3T can be attributed to several factors. First, its short bore (125 cm) allows for good visibility for brain exams via the rear-facing mirror mounted on the head coil. Second, when the subject’s brain is being imaged, their hands remain outside the bore, free to move laterally. Finally, for a lower extremity scan (e.g., a knee) the patient’s entire torso remained outside the bore.
A limitation of the study is the comparison was conducted on 60-cm bore whole body scanners, as opposed to 70-cm wide bore 3T scanners, which are also available at our institution. The 60-cm bore scanner was selected for this study because its main purpose was to compare image quality between the whole-body and compact scanners. As the C3T already offers 3.5 times the maximum slew rate of the 60-cm bore scanner, the 70-cm bore system (33 mT/m 150 T/m/s) was rejected for this study, since the slew rate discrepancy would have been even more pronounced, and potentially biased the image quality comparison.
Conclusion
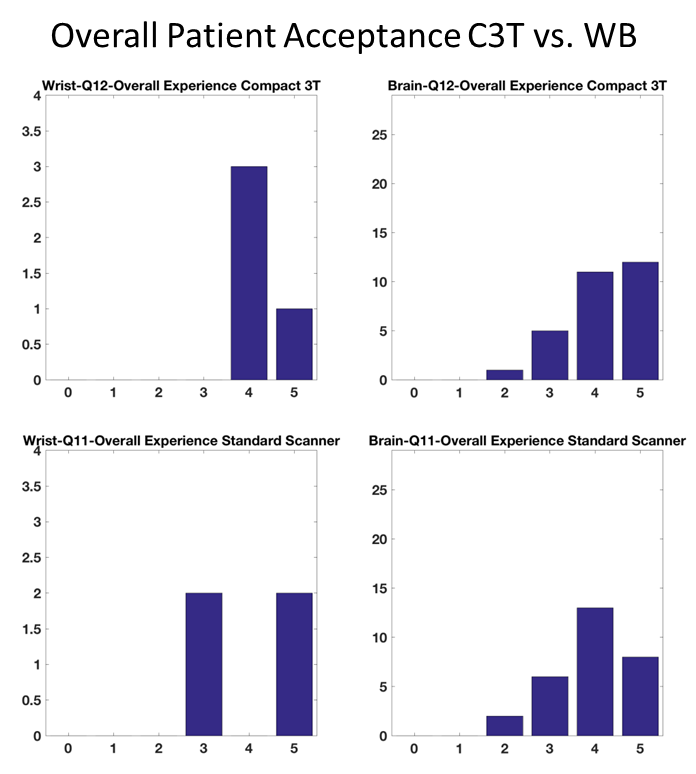
In most categories, the level of patient acceptance for the C3T scanner was significantly superior to a whole-body MR scanner. Study participants reported a positive overall experience in the C3T, and the majority of the subjects preferred the C3T over a 60-cm inner diameter whole-body system (Fig 5). Patient comfort is an important design consideration when developing MR scanners and the compact architecture performs very well in this area.
Acknowledgements
This work was supported by NIH grants U01 EB024450-01 and BRP RO1EB010065.References
1. Foo TKF, Tan ET, Schenck JF, Graziani D, Laskaris E, Vermilyea M, et al. Novel High Performance, Compact 3.0T MRI System for Imaging the Brain. Mil.Heal. Syst. Res. Symp., Orlando: 2016.
2. Weavers PT, Shu Y, Tao S, Huston J, Lee S-K, Graziani D, et al. Technical Note: Compact three-tesla magnetic resonance imager with high-performance gradients passes ACR image quality and acoustic noise tests. Med Phys 2016;43: 1259-64. doi:10.1118/1.4941362.
3. Weavers PT, Campeau NG, Shu Y, Tao S, Trzasko JD, Gray EM, Foo TK, Bernstein MA, Huston J. Improved T2-weighted 3D FLAIR from a compact, lightweight 3T scanner with high performance gradients. ISMRM Annu. Meet., Honolulu, Hawaii:2017.
4. Lee S-K, Mathieu J-B, Graziani D, et al. Peripheral nerve stimulation characteristics of an asymmetric head-only gradient coil compatible with a high-channel-count receiver array. Magn Reson Med 2016;76:1939–1950. doi: 10.1002/mrm.26044.
Figures