2630
Do MRI structured reports for diabetic foot contain concise information for clinical application?1Department of Radiology, Peking University First Hospital, Beijing, China, 2Department of Plastic Surgery & Burn, Peking University First Hospital, Beijing, China, 3Department of Biostatistics, Peking University First Hospital, Beijing, China
Synopsis
The aim of this study is to evaluate if structured reporting of MRI in diabetic foot(DF) contain concise information for clinical application compared with nonstructured reporting. Thirty nonstructured foot MRI reports of patients with DF were included, and another structured report was written for each patient. Three readers (A, B&C) evaluated the nonstructured and structured reports. Statistical analysis included Wilcoxon signed ranks tests and chi-square tests. All readers needed shorter time to understand the structured reports. For the 8 features for DF, two readers could understand bone edema significantly more often when reading structured versus nonstructured reports. All readers needed to evaluate images when reading nonstructured reports, 2 radiologists (reader A&C) needed to evaluate images when reading structured reports, and reader B(doctor of burn & plastic surgery) only needed 4(13.3%) to evaluate images when reading the structured reports. All readers missed Charcot joint and fracture when reading nonstructured reports, but only reader A missed fracture and reader C missed Charcot joint when reading structured reports. All readers found another abscess when reading structured reports. In conclusion, structured reports of MRI in patients with DF provided more concise information for clinical application than nonstructured reports.
INTRODUCTION
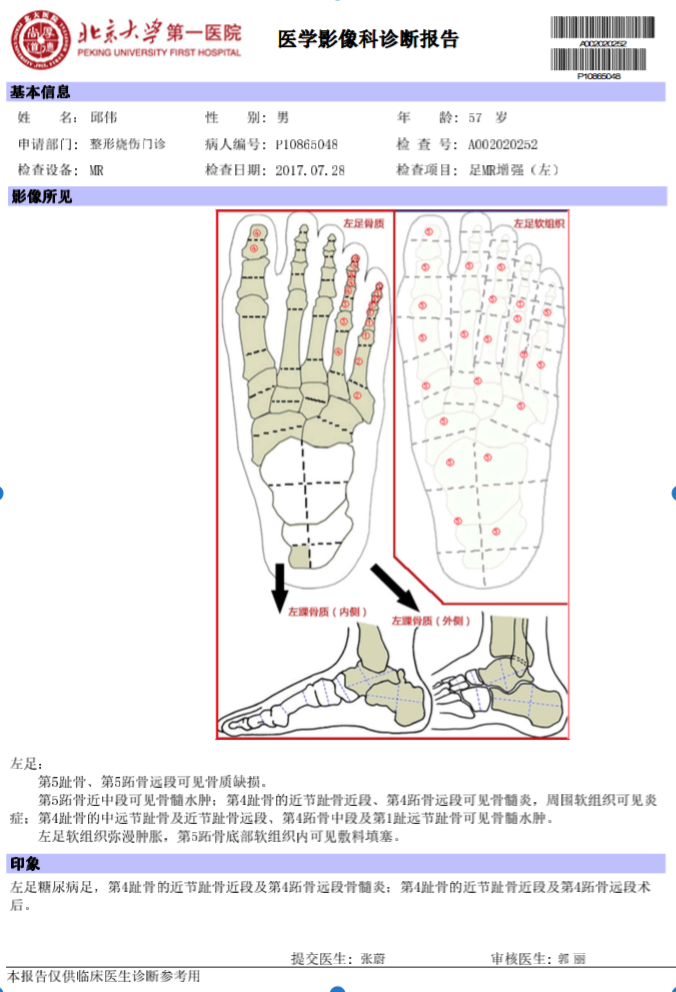
MR imaging can be quite useful in the evaluation of complications related to the diabetic foot.1-3 Few data are available on how often MRI structured reports provide concise information for clinical application in patients with diabetic foot (DF).4,5 The aim of this study is to evaluate if structured reporting of MRI in DF contain concise information for clinical application compared with nonstructured reporting.METHODS
Conventional nonstructured foot MRI reports of patients with DF were included, and another structured report was written for each patient after implementation of a structured reporting template. Three readers, two radiologists (Reader A & C), and one doctor of burn & plastic surgery (Reader B), evaluated the reports to assess lesion load, presence of 8 features for DF, and necessity to review MR images for understanding the reports. The time that each reader was needed to read and understand the reports was recorded. Statistical analysis included Wilcoxon signed ranks tests and chi-square tests.RESULTS
Thirty structured and nonstructured reports were reviewed. All readers needed shorter time to understand the structured reports (p = 0.008, p = 0.007 and p < 0.001). For the 8 features for DF, two readers(Reader B&C)could understand bone edema significantly more often when reading structured versus nonstructured reports (p =0.013, p = 0.008). Reader A could understand lesion load(Osteomyelitis and soft tissue infection)significantly more often when reading structured versus nonstructured reports (p = 0.037, p < 0.001). Reader C could understand ulcer or sinus significantly more often when reading structured versus nonstructured reports (p = 0.007). All readers needed to evaluate images when reading nonstructured reports, 2 radiologists needed to evaluate images when reading structured reports, and reader B only needed 4(13.3%) to evaluate images when reading the structured reports. There was only one case each with Charcot joint, fracture, and dislocation of joint, and 2 cases with abscess. All readers missed Charcot joint and fracture when reading nonstructured reports, but only reader A missed fracture and reader C missed Charcot joint when reading structured reports. All readers found another abscess when reading structured reports.DISCUSSION
Our study showed that, in our practice, using SR could shorten the time of understanding MR reports for diabetic foot. And several findings deemed important for management of patients with DF were found more often in SR than in NSR for diabetic foot MRI. Lesion load(Osteomyelitis and soft tissue infection), bone edema, and the presence of ulcer or sinus were reported more frequently in SR than in NSR. The doctor of burn & plastic surgery rarely needed to evaluate MR images when reading the structured reports.CONCLUSION
Structured reports of MRI in patients with DF provided more concise information for clinical application than nonstructured reports.Acknowledgements
We thank Suisui Zhang & Xin Yue (Beijing Smart Tree Medical Technology Co. Ltd.) in the contribution of establishing MR structured reports.References
1.Russell JM, Peterson JJ, Bancroft LW. MR imaging of the diabetic foot. Magn Reson Imaging Clin N Am. 2008 Feb; 16(1): 59-70.
2.Low KT, Peh WC. Magnetic resonance imaging of diabetic foot complications. Singapore Med J. 2015 Jan; 56(1): 23-33; quiz 34.
3.McCarthy E, Morrison WB, Zoga AC. MR Imaging of the Diabetic Foot. Magn Reson Imaging Clin N Am. 2017 Feb; 25(1): 183-194.
4.Larson DB, Towbin AJ, Pryor RM, et al. Improving consistency in radiology reporting through the use of department-wide standardized structured reporting. Radiology 2013; 267:240-250.
5.Johnson AJ, Chen MYM, Zapadka ME, et al. Radiology report clarity: a cohort study of structured reporting compared with conventional dictation. J Am Coll Radiol 2010; 7:501-506.
Figures