2593
Can MR elastography be used to measure liver stiffness in patients with iron overload?1Radiology, CHOP, Philadelphia, PA, United States, 2Radiology, CCHMC, Cincinnati, OH, United States
Synopsis
Untreated, iron overload causes hepatic fibrosis and cirrhosis, diabetes mellitus, hypogonadism, cardiomyopathy, dysrhythmias, and sudden death. In patients with liver iron overload, GRE based MRE techniques most likely fail due to very low signal from the liver. 2D Spin echo echo planar imaging (SE-EPI) based sequences have higher wave SNR compared with 2D GRE based MR elastography because of a higher number of wave cycles encoded per trigger (60 wave cycles per trigger vs three wave cycles per trigger in the typical 2D GRE acquisition sequence), which enables higher signal-intensity sampling of the phase waveform used to calculate the shear stiffness. In this study, our goal was to assess and demonstrate the applicability of a modified short TE, SE-EPI based MRE for staging liver fibrosis in select patients with liver iron overload conditions.
Purpose
Gradient recalled echo (GRE) based MRE is FDA approved and clinically available on atleast 3 major MR vendor platforms. However, in patients with liver iron overload, GRE based MRE techniques most likely fail due to very low signal from the liver at its current setting of echo time (TE). Additionally, presence of iron is inherently a paramagnetic substance that causes local disturbances in the magnetic field, shortening T2 and T2* relaxation times and consequently causing MR image signal loss. 2D Spin echo echo planar imaging (SE-EPI) based sequences have higher wave SNR compared with 2D GRE based MR elastography because of a higher number of wave cycles encoded per trigger (60 wave cycles per trigger vs three wave cycles per trigger in the typical 2D GRE acquisition sequence), which enables higher signal-intensity sampling of the phase waveform used to calculate the shear stiffness. More recently, a short TE, SE-EPI based MRE technique was introduced with improved signal-to-noise and scan efficiency that allowed for rapid acquisition of elastography of the chest within 1 to 2 breath-holds. An implementation of short TE SE-EPI MRE was developed to overcome signal loss because of susceptibility in all but the most severely iron-overloaded patients. The design of this acquisition sequence enables the use of a very low TE that can in-turn allow this technique to reliably assess fibrosis in patients with liver iron overload. In this study, our goal was to assess and demonstrate the applicability of a modified short TE, SE-EPI based MRE for staging liver fibrosis in select patients with liver iron overload conditions.Methods
Patients were referred for routine clinical MRI scans for evaluation of hepatic iron overload. MRE was performed as part of the routine clinical MRI exam in these patients. A modified, short TE, SE-EPI based MRE was performed in 43 patients referred for liver iron overload evaluation. Patients were asked to arrive fasting for a minimum of four hours to reduce possible physiologic confounding effects. MR examination MRI scans were obtained on a Signa HDxt 1.5T software version HD 23 (GE Helathcare, Waukesha, WI, USA) equipped with a gradient system with a maximum amplitude of 33 mT/m and a 150 mT/m/msec slew rate using MR Touch hardware for MRE scans (GE Healthcare). MRE Imaging was performed using a modified short TE SE-EPI sequence.Results
Our patient cohort included 43 subjects (13 males; 30 females) with a mean age of 11.7 years (range: 2.7 to 21.0 years). Clinical characteristics of the patients who underwent MRE are summarized. β-thalassemia and Sickle Cell Anemia was the most common underlying disease occurring in 11 and 20 number of the patients respectively. Liver iron range was from 1.36 to 17.42 mg/gm (mean = 6.10 mcg/gm; median = 4.91 mcg/gm). MRE was successful in 33 patients and failed in 10 patients. In the successful MRE of 33 patients, liver stiffness ranged from 1.35 kPa to 4.47 kPa (mean = 2.15 kPa; median = 2.11 kPa). Of the 10 patients with failed MRE, 8 patients were with Sickle Cell Anemia and 2 patients were with β-thalassemia. Liver iron range of patients with failed MRE (n=10) was from 6.18 to 17.42 mg/gm (mean = 12.99 mcg/gm; median = 13.78 mcg/gm).Discussion and Conclusion
Our study has shown noteworthy observations in pediatric and young adults with liver iron overload. We have shown that a modified low TE, SE-EPI based MRE technique can measure liver stiffness in patients with iron overload upto 17.42 mg/gm. Our results suggests that SEEPI based MRE has the potential to fulfil a critical unmet need of evaluating fibrosis in patients with hemochromatosis and hence avoiding the need for unnecessary biopsies.
A modified, short TE, SE-EPI based MRE method offers as a reliable alternative to assess liver fibrosis in this patient population. In our patients, we were able to successfully use SE-EPI based MRE to measure liver stiffness for fibrosis assessment in patients with liver iron upto 17.42 mg/gm.
Acknowledgements
No acknowledgement found.References
Serai SD, Trout AT, Sirlin CB (2017) Elastography to assess the stage of liver fibrosis in children: Concepts, opportunities, and challenges. Clinical Liver DiseaseFigures
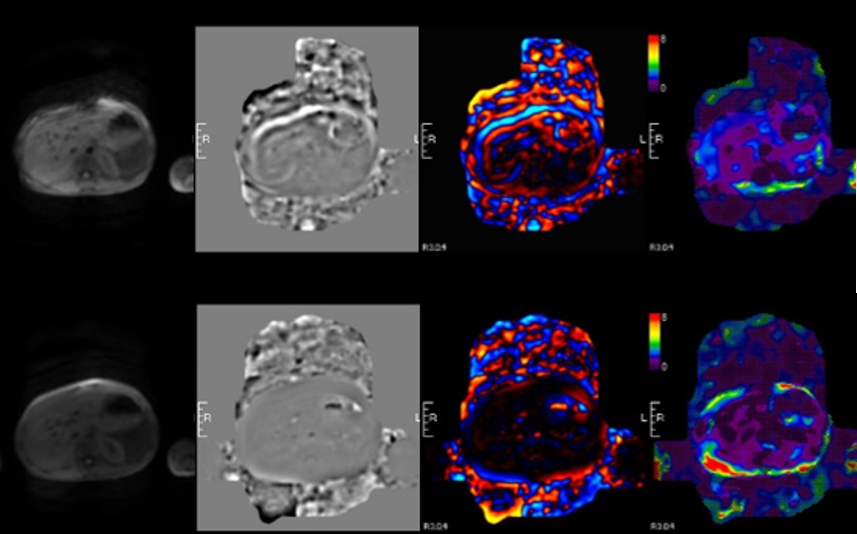
Top row: successful MRE of a patient with iron overload; from left to right - Magnitude, Phase, Color wave and color stiffness map. Waves can be seen in the liver region on the phase and color wave images. Stiffness map has areas of measurable stiffness areas.
Bottom row: Failed MRE. Phase and color wave images are blank with no waves. Stiffness maps has no areas of measureable stiffness.