2552
Expanding the limits of cardiovascular MR: amyloid detection in the liver and spleen1CMR department, National Amyloidosis Center, UCL Royal Free Hospital, London, United Kingdom, 2Internal Medicine, Università degli Studi di Pavia, Pavia, Italy, 3National Amyloidosis Center, UCL Royal Free Hospital, London, United Kingdom, 4Barts Health - Barts Heart Centre, London, United Kingdom, 5National Institute of Health, Washington, MD, United States
Synopsis
In this study we evaluated the utility of bolus-only ECV maps in extra-cardiac AL amyloidosis by comparing it with SAP scintigraphy findings in liver and spleen. These two techniques where performed in a large prospective cohort of patients with suspected systemic AL amyloidosis and where compared in terms of (1) diagnostic accuracy in liver and spleen amiloidosis; (2) quantification of the liver and spleen amyloid deposits. This was done using a standard acquisition for cardiac studies, with no extra image acquisition or optimization for hypochondriac regions.
Introduction
Systemic amyloidosis is a disease characterized by amyloid infiltration into different organs and tissues. CMR is the reference standard to assess cardiac amyloid infiltration, that can be visualized with LGE and measured with ECV mapping. The utility of ECV mapping in detecting and quantifying amyloid in other organs has never been investigated.
Aim
The aim of this study is to assess, in a large prospective cohort of patient suspected systemic amyloidosis, the ability of ECV mapping to detect amyloid infiltration in the liver and spleen. This was done using standard acquisition for cardiac studies, with no extra image acquisition.Methods
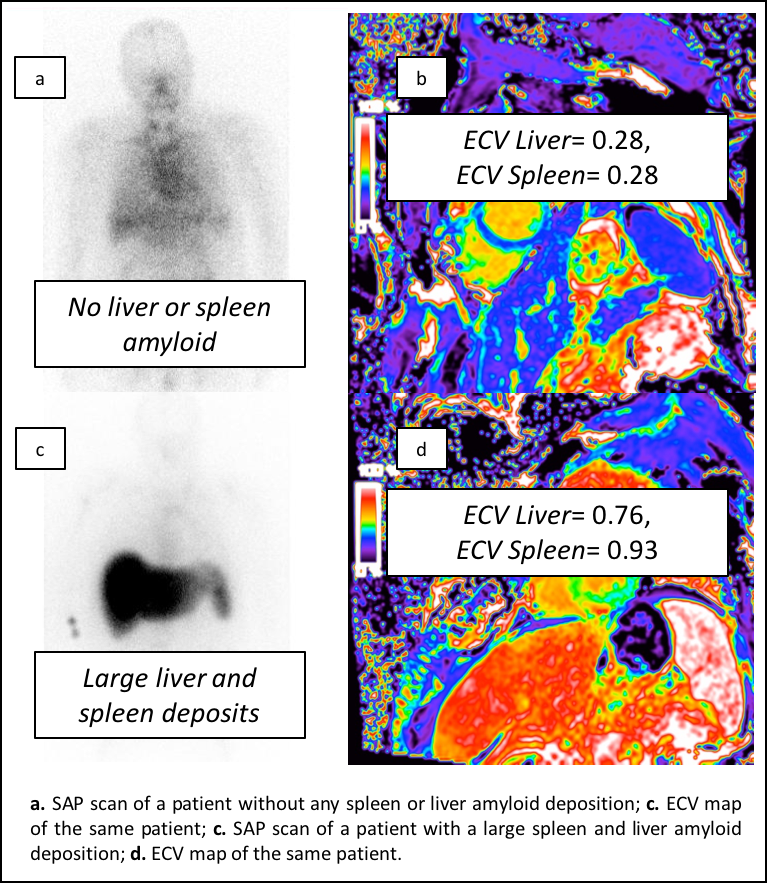
732 consecutive patients with suspected systemic amyloidosis were prospectively enrolled in the study between 2015 and 2017. All patients underwent scintigraphy with 123I-labeled serum amyloid P component (SAP scan), the reference standard for assessment of the amyloid burden in the spleen and liver: the uptake in the spleen and liver was classified in five categories (no amyloid, uncertain, small, medium, large). All patients underwent a standard cardiac MR protocol including acquisition of three short axis slices with pre and post contrast T1 mapping (by Modified Look-Locker Inversion recovery, MOLLI) and online ECV mapping reconstruction. The liver and spleen ECV was measured on the ECV maps acquired for the left ventricular short axis (Figure 1).Results
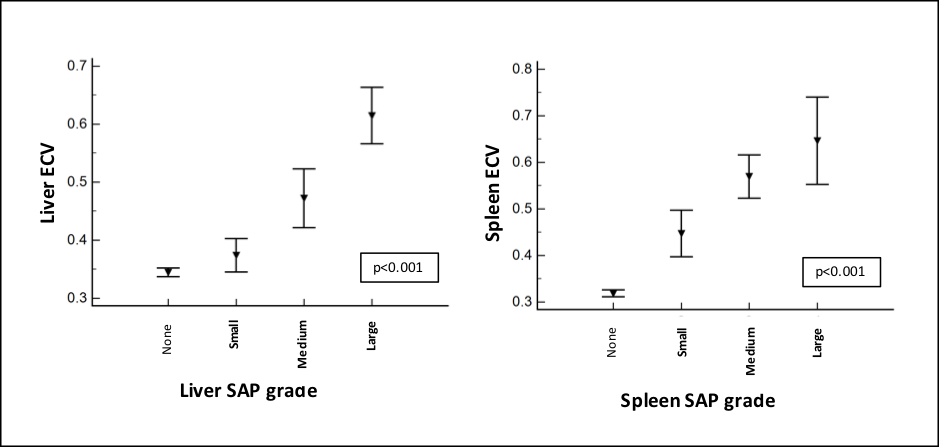
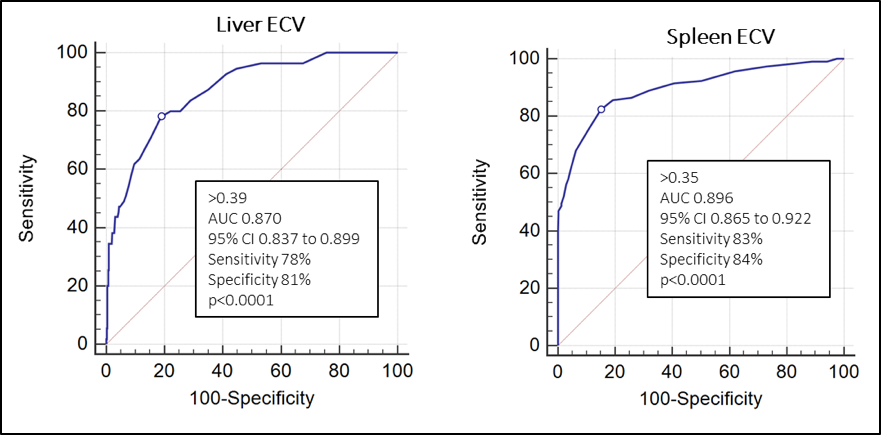
There was a good correlation between ECV and amyloid burden in the liver and spleen as assessed by SAP scintingraphy (Spearman's coefficient of rank correlation: 0.465 (liver), 0.603 (spleen), p<0.0001) (Figure 2). The ECV showed a very good diagnostic accuracy to detect amyloid in the liver (AUC 0.870; 95% CI 0.837 to 0.899; sens 78%, spec 81%) and in the spleen (AUC 0.896; 95% CI 0.865 to 0.922; sens 83%, spec 84%) (both p<0.0001) (Figure 3).Conclusions
CMR has an excellent diagnostic accuracy for the detection of amyloid in the spleen and liver. This does not require any additional image acquisition and can therefore be easily integrated in the routine clinical practice. ECV of the liver and spleen could significantly improve the diagnostic pathway for extra-cardiac amyloid but also has the potential to become an important tool to monitor treatment response.Acknowledgements
No acknowledgement found.References
No reference found.Figures