2543
Validation of a radiomics nomogram for preoperative prediction of early recurrence in hepatocellular carcinoma less than 5cm1Diagnostic Radiology, National Cancer Center/ Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China, 2GE Healthcare, China, Beijing, China
Synopsis
A high early recurrence (ER) (≤ 1 year) rate of hepatocellular carcinoma (HCC) remains a significant concern. It is an important problem to find a powerful preoperative tool for predicting ER. This study aimed to development and validation of a Radiomics Nomogram for Preoperative Prediction ER in hepatocellular carcinoma less than 5cm. We found that the textural signature was a significant predictor for ER in HCC, and Radiomics nomogram performed better for preoperative prediction of ER in HCC.
Introduction: A high early recurrence (ER) (≤ 1 year) rate of hepatocellular carcinoma (HCC) remains a significant concern[1]. It is an important problem to find a powerful preoperative tool for predicting ER[2-3]. This study aimed to development and validation of a Radiomics Nomogram for Preoperative Prediction ER in hepatocellular carcinoma less than 5cm.
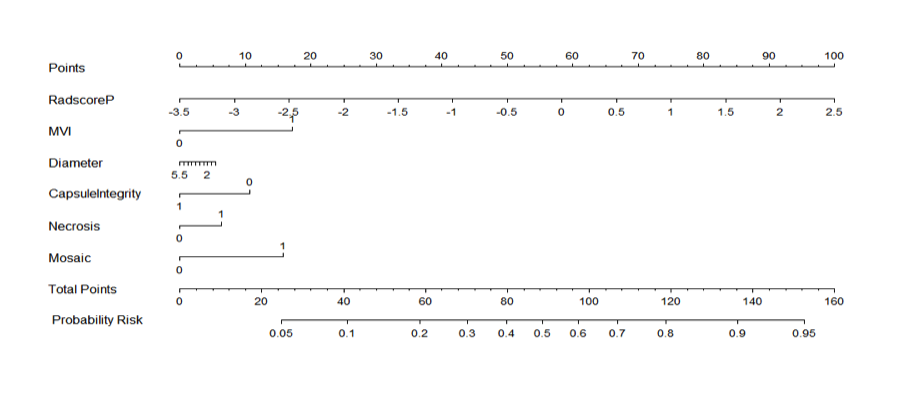
Materials and methods: A total of 110 HCC patients with primary solitary HCC measuring less than 5 cm in diameter, who underwent partial hepatectomy were enrolled in this retrospective study. And all the patients were followed up more than 1 year. Preoperative clinical factors associated with ER were evaluated. Texture features were extracted from arterial phase (AP) and portal venous phase (PP) CEMR images. Followed the feature selection, multivariate logistic regression analysis was applied for modeling , including a clinical factor (CF) model, an AP textural feature model, a PP textural feature model and a combined model. The area under the curve (AUC)s of operating characteristics (ROC) of the above models were used to explore their performance to discriminate ER respectively. The best model was selected and a nomogram was obtained. Both clinical parameters(p<0.05) and the radiomics signature score were conducted for multivariate logistic regression and a nomogram was generated by using the rms package of R, version 3.4.1 (http://www.r-project.org/).
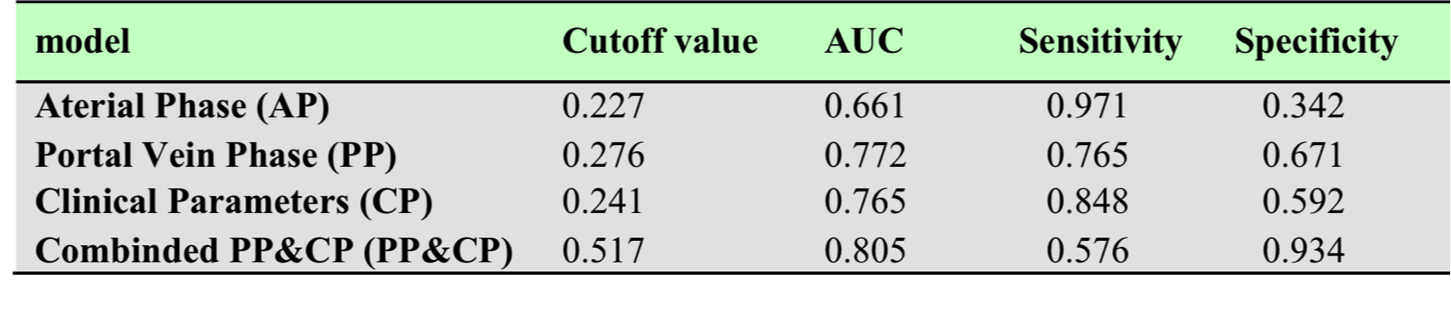
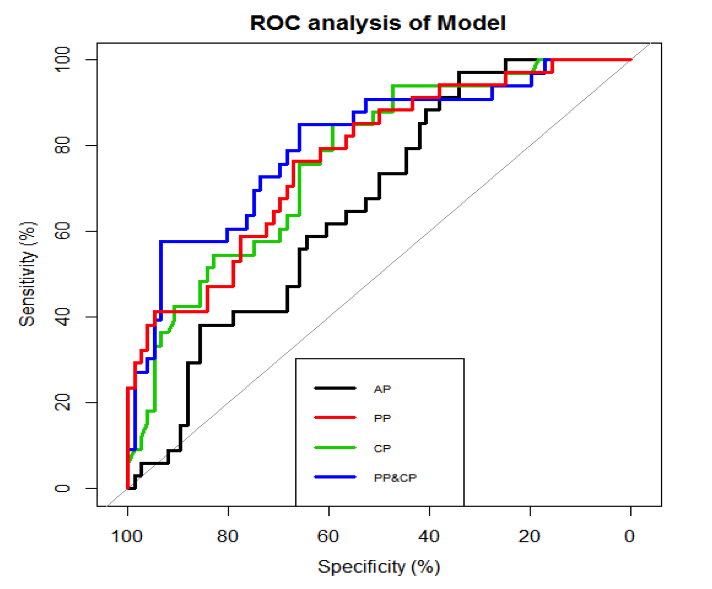
Results: The significant textural features of CF, AP, PP chosen from 68 candidate features were 5, 2 and 10, respectively (P<0.05). The PP model presented better performance than AP- and CF- model in the discrimination of ER alone with an AUC of 0.765, 0.661, 0.772; sensitivity of 0.848, 0.971, 0.765; specificity of 0.592, 0.342, 0.671. Adding a PP textural signature into conventional clinical variables can significantly improve the accuracy of the preoperative model in predicting ER (AUC of 0.805, sensitivity of 0.576, specificity of 0.934, cutoff value of 0.517).
Conclusions: The textural signature was a significant predictor for ER in HCC. Radiomics nomogram performed better for preoperative prediction of ER in HCC.
Acknowledgements
none.References
1. Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015, 136(5): E359-386.
2. Li T, Qin LX, Gong X, et al. Clinical characteristics, out-come, and risk factors for early and late intrahepatic recurrence of female patients after curative resection of hepatocellular carcinoma. Surgery. 2014, 156(3): 651-660.
3. Li T, Wang SK, Zhou J, et al. Positive HBcAb is associated with higher risk of early recurrence and poorer survival after curative resection of HBV-related HCC. Liver Int. 2016, 36(2): 284–292.
Figures