2526
Development of a fast 4D-MRI with sub-second volumetric frame rate for respiratory motion tracking in abdominal radiotherapy1Medical physics and research department, Hong Kong Sanatorium & Hospital, Happy Valley, Hong Kong
Synopsis
Time-resolved volumetric MRI (4D-MRI) is gaining more interests for better tumor motion characterization than 4D-CT in abdominal radiotherapy, while 3D sequence has limited use for 4D-MRI acquisition due to its slow volume-frame-rate (VFR) and various motion artifacts. We developed a fast 4D-MRI technique based on CAIPIRINHA accelerated 3D spoiled gradient echo sequence and a 1.63 frames-per-second (615ms/frame, ~1/7 of normal respiratory cycle of 4-5s) VFR was achieved. This 4D-MRI was demonstrated for whole abdomen respiratory motion tracking in healthy volunteers, indicating its great potentials for internal-target-volume definition in radiotherapy treatment planning and image guidance of MR-guided-radiotherapy.
Introduction
Time-resolved volumetric MRI (4D-MRI) has been gaining more interests for better tumor motion characterization than 4D-CT in chest and abdomen radiotherapy (RT) (1,2). 2D acquisition, either in interleaved multi-slice or orthogonal cine acquisition mode, is frequently used for 4D-MRI because 3D acquisition was thought still slow to capture the respiratory motion in chest and abdomen, and also associated with various motion artifacts. However, 2D acquisition suffers from anatomical structure discontinuity (structure missing and/or zigzag edge) even after long acquisition and dedicated respiratory-phase sorting despite of its fast acquisition per slice (1). Thus, we prompt to develop a 4D-MRI technique with sub-second volumetric frame rate (VFR) for whole abdominal motion tracking for RT applications.Methods
3D spoiled gradient-echo sequence accelerated with CAIPIRINHA (Controlled aliasing in parallel imaging results in higher acceleration) was developed. A short TR of 1.57ms was achieved by using wide receiver bandwidth (RBW), maximal gradient slew-rate and asymmetric echo. This imaging protocol (transversal, FOV=350(FE)x262.5(PE)mm, thickness=4mm, matrix size=128x128x56, TE/TR=0.53/1.57ms, flip-angle=5o, RBW=1400Hz/voxel, CAIPIRINHA factor=4, partial Fourier factor=6/8) resulted in a temporal resolution of 615ms per volume (56 slices), i.e. 1.63 fps (frames-per-second) and a reconstructed voxel size of 2.7x2.7x4mm. This 4D-MRI protocol was applied for abdominal imaging of 5 healthy volunteers on a 1.5T MRI scanner dedicated for RT. Subjects were immobilized on a personalized vacuum cushion overlaid on a flat RT-indexed couch top. An 18-channel body matrix coil and spine coil were used for acquisition. 144 dynamics of the volume, in total 8064 images, were acquired in 89s. During free-breathing acquisition, respiratory curve was logged and its time stamp was corresponded to that of acquired MR images. The motions of liver dome, kidneys and spleen were analyzed using 3D-slicer. Their correlation to respiratory curve was also demonstrated.Results
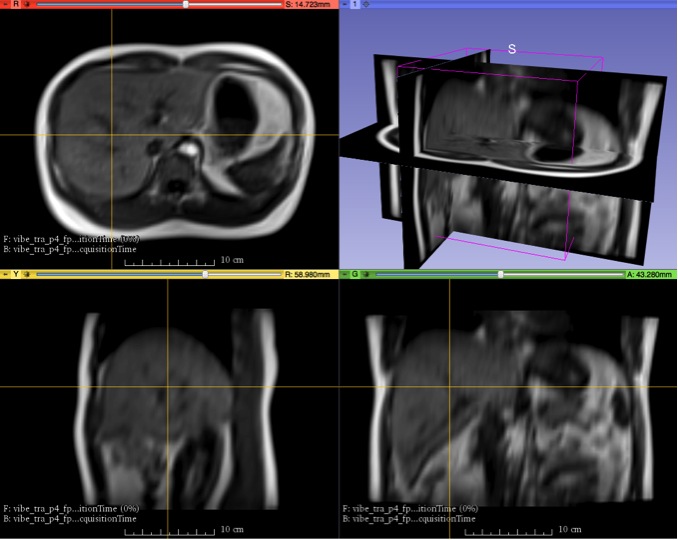
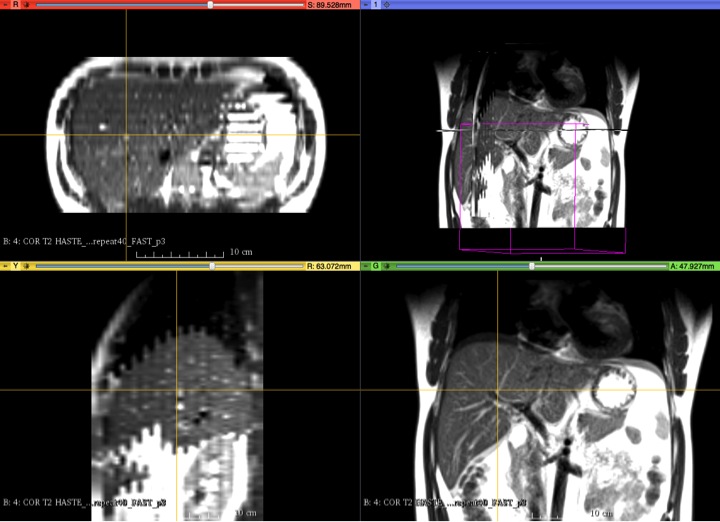
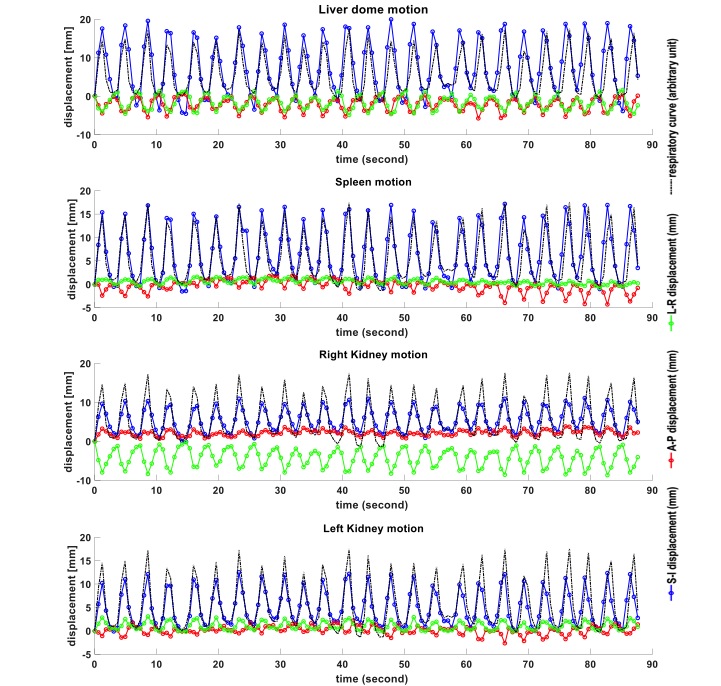
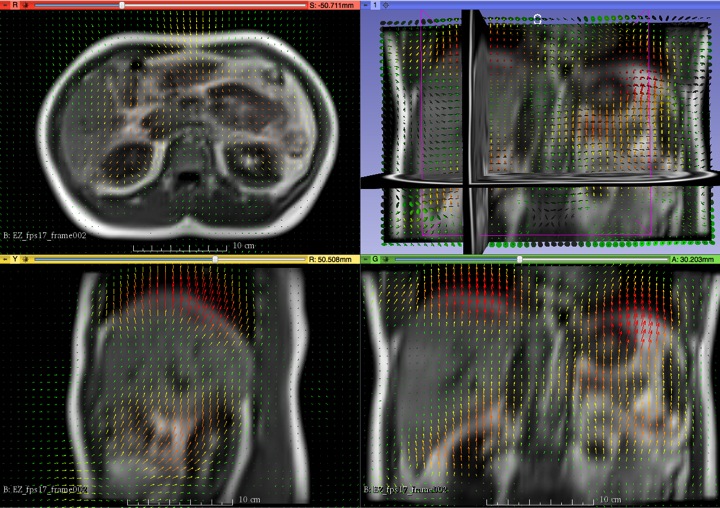
The reformatted 4D-MRI images of a volunteer were illustrated in Fig. 1 and compared to 2D-HASTE-based 4D-MRI images (30slices to cover whole abdomen, coronal, voxel size = 2.3x2.3x6 mm, 165ms/slice yielded ~5s/volume) in Fig.2. Even at a relatively fast respiratory cycle of ~3.3s, the respiration induced blurring was observable but still minor at diaphragm in SI direction on sagittal and coronal views (Fig. 1). There was no ghosting artifact and the cardiac motion effect on liver image quality was small. In contrast, 2D-HASTE images showed severe zigzag artifacts on reformatted sagittal and transversal images although its coronal resolution was better. The displacements of liver dome, kidneys and spleen relative to the first frame in three orthogonal directions along with the logged respiratory curve were illustrated in Fig. 3. The motion vectors of the whole abdomen (frame 2 relative to frame 1) were shown in Fig. 4.Discussion
We developed a 4D-MRI based on 3D gradient-echo acquisition and a VFR of 1.63fps (615ms/volume, ~1/7 of normal respiratory cycle of 4-5s) was achieved enabling of whole abdomen motion tracking. Transversal acquisition was adopted in this study to comply with 4D-CT. VFR of this 4D-MRI could be further increased straightforwardly by adjusting volume matrix size, acquisition orientation when targeting for small volume tracking. This fast 4D-MRI technique could be potentially used for various scenarios in abdominal RT applications. For treatment planning, it is helpful to define internal-target-volume (ITV) by assessing 3D motion trajectories of the tumor. It is worth noting that spatial resolution and VFR of this 4D-MRI could be further improved by integrating other accelerations techniques like non-Cartesian under-sampling and compressed sensing (3,4). It also has potentials for real-time motion monitoring and radiation delivery guidance for MR-guided-radiotherapy (MRgRT) (5), particularly for large and irregular-shaped tumors in which case 2D MR acquisition is difficult for whole tumor tracking. For this purpose, the acquisition speed is thought sufficiently fast but the bottlenecks become image reconstruction (tens of seconds delay was observed on our MRI console), visualization, on-line tracking algorithm and interaction with linear accelerator. This study has limitations. Limited numbers of healthy volunteers instead of real patients were included. The robustness of this 4D-MRI to faster respiration and highly irregular motion (like cough) needs to be further studied. Study of combining with other advanced acceleration techniques like compressed sensing to pursue higher spatial-temporal resolution is under way.Conclusion
A fast 4D-MRI based on 3D gradient-echo acquisition was developed and demonstrated for whole abdomen respiratory motion tracking. This technique has potentials for ITV definition in treatment planning of abdomen RT as well as image guidance of MR-guided-radiotherapy.Acknowledgements
No acknowledgement found.References
1. Schmidt MA, Payne GS. Radiotherapy planning using MRI. Phys Med Biol 2015;60(22):R323-361.
2. Biederer J, Hintze C, Fabel M, Dinkel J. Magnetic resonance imaging and computed tomography of respiratory mechanics. J Magn Reson Imaging 2010;32(6):1388-1397.
3. Deng Z, Pang J, Yang W, et al. Four-dimensional MRI using three-dimensional radial sampling with respiratory self-gating to characterize temporal phase-resolved respiratory motion in the abdomen. Magn Reson Med 2016;75(4):1574-1585.
4. Feng L, Grimm R, Block KT, et al. Golden-angle radial sparse parallel MRI: combination of compressed sensing, parallel imaging, and golden-angle radial sampling for fast and flexible dynamic volumetric MRI. Magn Reson Med 2014;72(3):707-717.
5. Lagendijk JJW, Raaymakers BW, Raaijmakers AJE, et al. MRI/linac integration. Radiotherapy and Oncology 2008;86(1):25-29.
Figures