2525
Hepatobiliary phase imaging using optimized integrated combination with parallel imaging and compressed sensing technique.1Department of Radiology, Gifu University School of Medicine, Gifu, Japan, 2Department of Radiology Services, Gifu University Hospital, Gifu, Japan, 3Philips Japan, Tokyo, Japan
Synopsis
Gadoxetic acid-enhanced MRI plays an important role in the assessment of hepatic diseases. Hepatobiliary phase image has an amazing tissue contrast for the lesions with or without functional hepatocytes, however, which is still challenging for patients with limited breath-hold capabilities. We assessed prototype sequence using optimized integrated combination with parallel imaging and compressed sensing technique (Compressed-SENSE) for liver imaging. Our results demonstrated that Compressed-SENSE technique enabled significant reduction of acquisition time without image quality degradation resulting in higher spatial resolution and excellent image quality compared with conventional method.
Introduction
Gadoxetic acid-enhanced MRI is an essential modality for the assessment of hepatic diseases and is recommended in several guidelines1,2. A bolus injection of gadoxetic acid allows the assessment of tumor vascularity and hemodynamics through hepatic arterial to portal venous phase and enables excellent tissue contrast for the differentiation between lesions with and without functional hepatocytes in hepatobiliary phase, which is obtained 15-20 minutes after contrast administration3.
Recent technical innovations have been introduced to the liver MRI. Accelerated parallel imaging (PI) technique, as for instance SENSE (sensitivity encoding), can reduce acquisition time. In addition, the development of fat-suppressed 3-dimentional gradient echo T1-weighted imaging (e.g. eTHRIVE; enhanced T1 high resolution isotropic volume excitation) has contributed to imaging with a thinner effective slice thickness4. However, gadoxetic acid-enhanced MR imaging is still challenging for patients with compromised breath-hold capacity, such as young children or critically ill adults, resulting in degradation of image quality.
The compressed sensing (CS) image acquisition and reconstruction technique has recently been developed and applied in clinical settings5-8. In this study, we assessed prototype eTHRIVE sequence using optimized integrated combination with PI and CS technique (Compressed SENSE) for liver dynamic imaging. We hypothesized that the use of Compressed SENSE may contribute the improvement of image quality and spatial resolution during gadoxetic acid-enhanced hepatobiliary imaging. The purpose of this study was to evaluate the feasibility of Compressed SENSE technique in hepatobiliary phase imaging compared with conventional methods.
Methods
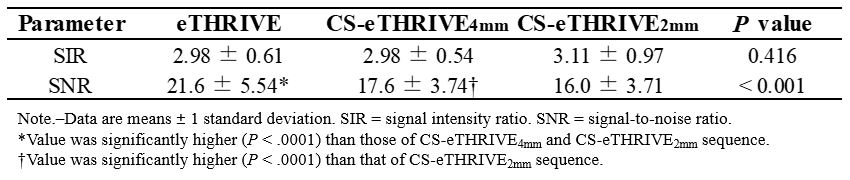
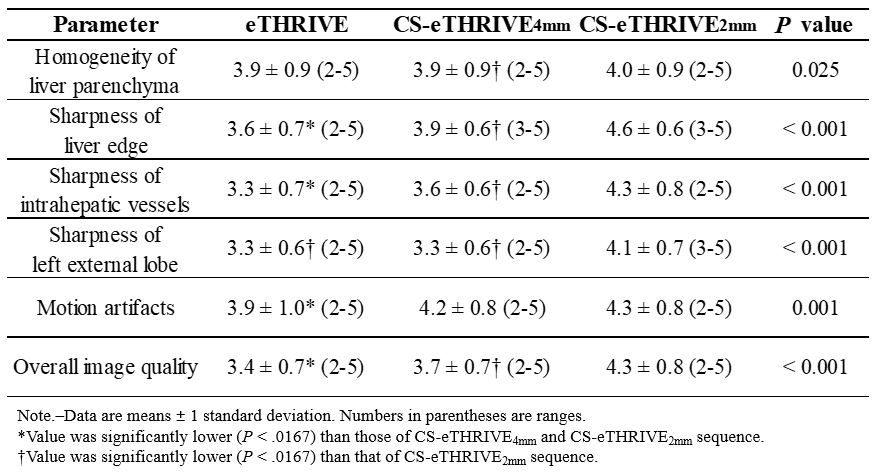
Institutional review board approval was obtained for this prospective HIPAA-compliant study. Sixty consecutive patients (41 men, 19 women, age range 27-84 years, mean age 64.1 years) with suspicious having liver disease underwent gadoxetic acid-enhanced MRI. All patients underwent hepatobiliary phase imaging with conventional breath-hold eTHRIVE with SENSE (eTHRIVE; SENSE factor, 1.75; slice thickness/gap, 4/-2mm; acquisition time, 20 sec), breath-hold eTHRIVE with Compressed SENSE (CS-eTHRIVE4mm; CS-SENSE factor, 3.4; 4/-2 mm; 10 sec), and thin-slice breath-hold eTHRIVE with Compressed SENSE (CS-eTHRIVE2mm; CS-SENSE factor, 3.4; 2/0 mm; 20 sec) at a 3-T clinical scanner (Ingenia CX; Philips Healthcare, Netherlands) with a 32-channel phased-array receiver coil. Three sequences of hepatobiliary phase imaging were obtained in random order 15-21 min (mean, 16.1 min) after an intravenous bolus injection of gadoxetic acid. For quantitative image analyses, signal intensity ratio (SIR) and signal-to-noise ratio (SNR) of liver parenchyma were calculated in each sequence. For qualitative image analyses, two radiologists coincidentally graded homogeneity of liver parenchyma, sharpness of liver edge, intrahepatic vessels and left external lobe, motion artifacts, and overall image quality using a five-point rating scale. Quantitative measurements and qualitative scales were compared between three sequences using repeated measures ANOVA/pairwise t-test with Bonferroni correction (BC) and Friedman test with pairwise Wilcoxson signed rank test with BC, respectively.Results
Quantitative results were demonstrated in Table 1. No significant difference was found in SIRs of liver parenchyma among three sequences. SNR of liver parenchyma in CS-eTHRIVE2mm (16.0) was slightly lower than that in eTHRIVE sequence (21.5) and in CS-eTHRIVE4mm (17.6) (P < 0.001). Qualitative results were demonstrated in Table 2. Sharpness of liver edge, intrahepatic vessels, left external lobe, and overall image quality in CS-eTHRIVE2mm sequence (4.6, 4.3, 4.1, 4.3) were significantly greater than those in eTHRIVE (3.6, 3.3, 3.3, 3.4) and those in CS-eTHRIVE4mm (3.9, 3.6, 3.3, 3.7) (P < 0.001).Discussion
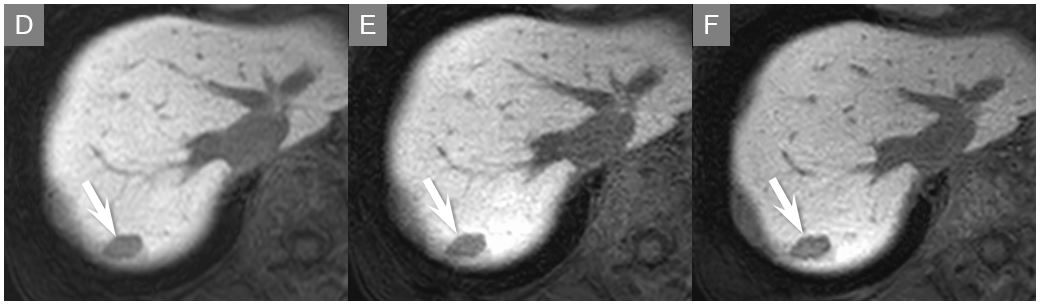
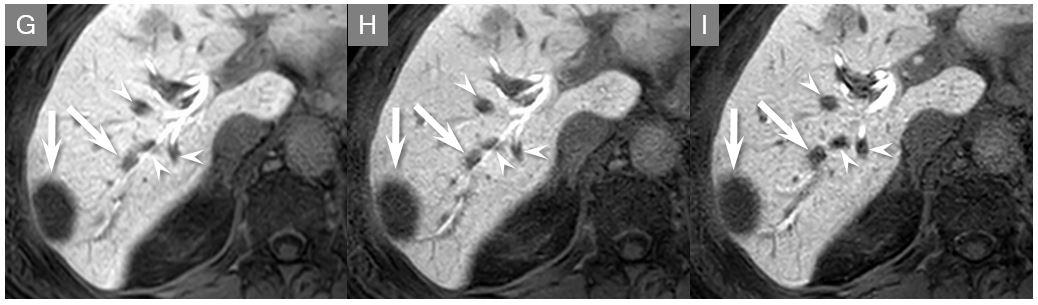
Our results demonstrated that Compressed-SENSE technique enabled double spatial resolution in CS-eTHRIVE2mm within the same breath-hold acquisition time (20 sec) as against conventional eTHRIVE (slice thickness/gap; 2/0 vs. 4/-2 mm). Due to the significant reduction of partial volume averaging effect and effective denoising algorithm of Compressed-SENSE, CS-eTHRIVE2mm sequence demonstrated overwhelming advantages in sharpness of liver edge, intrahepatic vessels, left external lobe, and overall image quality compared with eTHRIVE, with a very slight loss of SNR. We believe that CS-eTHRIVE2mm can contribute to the higher spatial resolution and better image quality for gadoxetic acid-enhanced hepatobiliary phase imaging.Conclusion
CS-eTHRIVE2mm sequence demonstrated the excellent spatial resolution and image quality with a slight loss of SNR in gadoxetic acid-enhanced hepatobiliary phase imaging.Acknowledgements
No acknowledgement found.References
1. Omata M, Cheng AL, Kokudo N, et al. Asia-Pacific clinical practice guidelines on the management of hepatocellular carcinoma: a 2017 update. Hepatology international 2017;11:317-70.
2. Kudo M, Matsui O, Izumi N, Iijima H, Kadoya M, Imai Y. Surveillance and diagnostic algorithm for hepatocellular carcinoma proposed by the Liver Cancer Study Group of Japan: 2014 update. Oncology 2014;87 Suppl 1:7-21.
3. Sano K, Ichikawa T, Motosugi U, et al. Imaging study of early hepatocellular carcinoma: usefulness of gadoxetic acid-enhanced MR imaging. Radiology 2011;261:834-44.
4. Goshima S, Noda Y, Kajita K, et al. Gadoxetic acid-enhanced high temporal-resolution hepatic arterial-phase imaging with view-sharing technique: Impact on the LI-RADS category. European journal of radiology 2017.
5. Kaltenbach B, Bucher AM, Wichmann JL, et al. Dynamic Liver Magnetic Resonance Imaging in Free-Breathing: Feasibility of a Cartesian T1-Weighted Acquisition Technique With Compressed Sensing and Additional Self-Navigation Signal for Hard-Gated and Motion-Resolved Reconstruction. Investigative radiology 2017.
6. Ono A, Arizono S, Fujimoto K, et al. Non-contrast-enhanced 3D MR portography within a breath-hold using compressed sensing acceleration: A prospective noninferiority study. Magnetic resonance imaging 2017;43:42-7.
7. Weiss J, Notohamiprodjo M, Martirosian P, et al. Self-gated 4D-MRI of the liver: Initial clinical results of continuous multiphase imaging of hepatic enhancement. Journal of magnetic resonance imaging : JMRI 2017.
8. Yoon JH, Yu MH, Chang W, et al. Clinical Feasibility of Free-Breathing Dynamic T1-Weighted Imaging With Gadoxetic Acid-Enhanced Liver Magnetic Resonance Imaging Using a Combination of Variable Density Sampling and Compressed Sensing. Investigative radiology 2017.
Figures