2524
Gadoxetic acid-enhanced dynamic MR imaging using optimized integrated combination with parallel imaging and compressed sensing technique.1Department of Radiology, Gifu University School of Medicine, Gifu, Japan, 2Department of Radiology Services, Gifu University Hospital, Gifu, Japan, 3Philips Japan, Tokyo, Japan
Synopsis
Gadoxetic acid-enhanced MRI represents an essential part in the assessment of hepatic diseases, however, dynamic imaging especially in hepatic arterial phase is still challenging for patients with limited breath-hold capabilities. We assessed prototype sequence using optimized integrated combination with parallel imaging and compressed sensing technique (Compressed-SENSE) for liver imaging, which enabled significant reduction of acquisition time resulting in excellent image quality with less motion artifact, especially in hepatic arterial phase, compared with conventional method. Our results demonstrated the significance and usefulness of Compressed-SENSE in clinical use for gadoxetic acid-enhanced dynamic MR imaging.
Introduction
Gadoxetic acid-enhanced dynamic magnetic resonance (MR) imaging is an essential modality for the assessment of hepatic diseases and is recommended in several guidelines1,2. Gadoxetic acid-enhanced dynamic imaging is commonly performed approximately 20-second-single breath-hold sequence using fat-suppressed 3-dimentional gradient echo T1-weighted imaging (e.g. eTHRIVE; enhanced T1 high resolution isotropic volume excitation) before and after gadoxetic acid contrast administration3. While present accelerated parallel imaging (PI) technique, as for instance SENSE (sensitivity encoding), can avoid respiratory motion artifacts by reducing acquisition time, patients with compromised breath-hold capacity, such as young children or critically ill adults, often cannot comply with breathing commands, leading to non-dynamic or even non-diagnostic studies. In addition, recent report suggests that the administration of gadoxetic acid reduces breath-hold capacity in the hepatic arterial phase and causes transient severe motion (TSM) artifacts4.
The compressed sensing (CS) image acquisition and reconstruction technique has recently been developed and applied in clinical settings5-7. We hypothesized that the reduction of acquisition time for dynamic liver MRI contributed to less motion artifacts and more acceptable image. In this study, we assessed prototype eTHRIVE sequence using optimized integrated combination with PI and CS technique (Compressed SENSE) for liver dynamic imaging. The purpose of this study was to evaluate the feasibility of Compressed SENSE technique in gadoxetic acid-enhanced dynamic MR imaging.
Methods
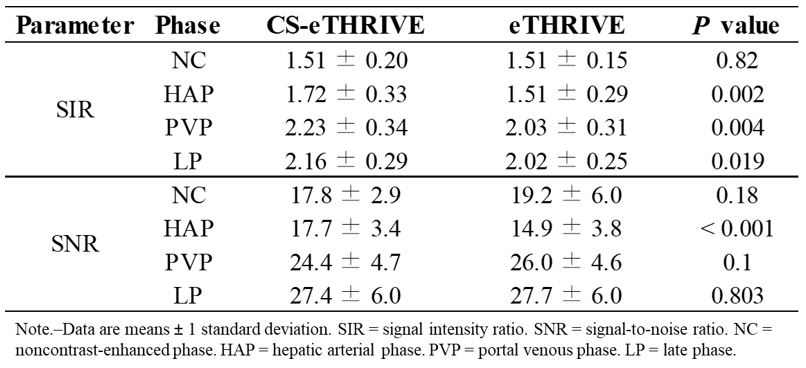
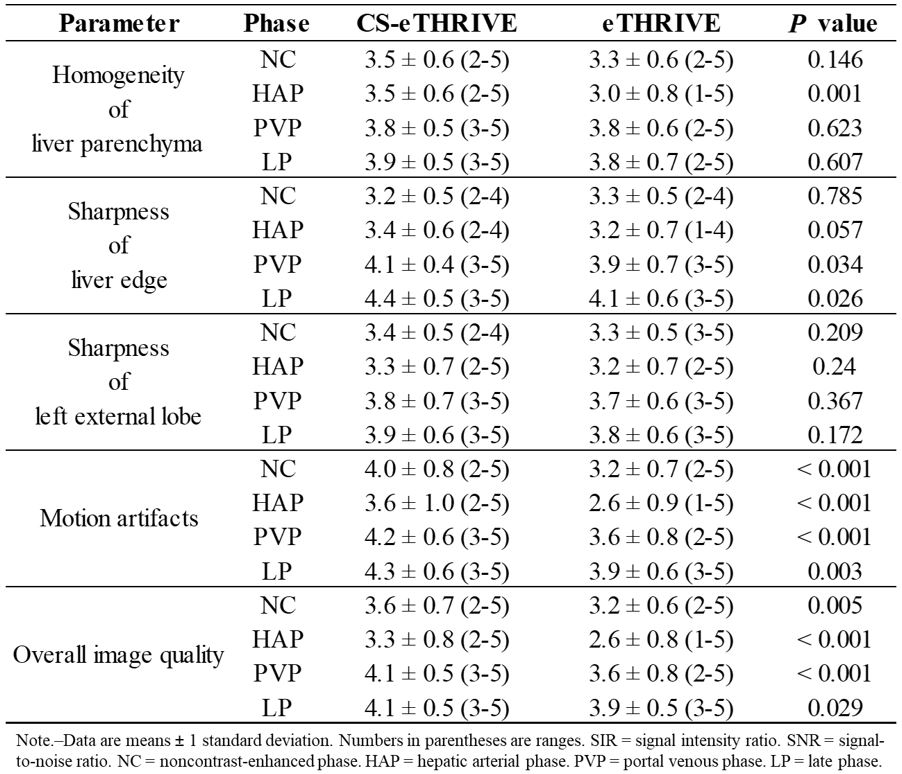
This prospective HIPAA-compliant study was approved by our institutional review board. Written informed consent was obtained from all patients. Forty-five patients underwent gadoxetic acid-enhanced dynamic imaging by eTHRIVE with Compressed SENSE (CS-eTHRIVE; CS-SENSE factor, 3.4; acquisition time, 10 sec) and were compared with propensity score-matched 45 patients who underwent conventional eTHRIVE with SENSE (eTHRIVE; SENSE factor, 1.75, acquisition time, 20 sec) at a 3-T clinical scanner (Ingenia CX; Philips Healthcare, Netherlands) with a 32-channel phased-array receiver coil. Propensity score matching was based on patients’ age, gender, body mass index, Child-Pugh score, and presence or absence of pulmonary emphysema and pleural effusion. After obtaining noncontrast-enhanced phase (NP) images, 0.1 mL/kg gadoxetic acid were administered with 30mL saline flush at a rate of 1mL/sec. Subsequently, contrast-enhanced dynamic images were obtained in hepatic arterial (HAP), portal venous (PVP), and late dynamic phase (LP) in 5, 45 and 115 second, respectively, after the peak aortic contrast enhancement detected by fluoroscopic bolus tracking system. For quantitative image analyses, signal intensity ratio (SIR) and signal-to-noise ratio (SNR) of liver parenchyma were calculated in each phase. For qualitative image analyses, two radiologists coincidentally graded homogeneity of liver parenchyma, sharpness of liver edge and left external lobe, motion artifacts, and overall image quality in each phase using a five-point rating scale. Unpaired t-test for quantitative measurements and Mann-Whitney U test for qualitative scales were performed to evaluate differences between two sequences.Results
Quantitative results were demonstrated in Table 1. SIRs of liver parenchyma with CS-eTHRIVE sequence were significantly higher than those with eTHRIVE in HAP (1.7 vs. 1.5), PVP (2.2 vs. 2.0), LP (2.2 vs. 2.0) (P < 0.019). SNR of liver parenchyma in HAP with CS-eTHRIVE sequence (17.6) was significantly higher than that with eTHRIVE (14.9) (P < 0.001). No significant difference was found between two sequences for SNR in NP, PVP, and LP. Qualitative results were demonstrated in Table 2. Homogeneity of liver parenchyma in HAP with CS-eTHRIVE sequence (3.6) was significantly better than that with eTHRIVE (2.6) (P < 0.001). Motion artifacts were significantly improved with CS-eTHRIVE sequence compared with eTHRIVE in all phases (P < 0.01). TSM artifacts in HAP was not observed in CS-eTHRIVE sequence (0%) but observed in eTHRIVE sequence (4.4%). Overall image quality with CS-eTHRIVE sequence was significantly better than that with eTHRIVE in all phases (P < 0.05).Discussion
Our results demonstrated that CS-eTHRIVE sequence reduced the breath hold acquisition time by half as against conventional eTHRIVE (10 vs. 20 sec) leading to less motion artifacts in all phases, especially in HAP. In fact, TSM artifacts in HAP was not observed in CS-eTHRIVE sequence compared with conventional eTHRIVE sequence (4.4%). In quantitative analysis, signal intensity of the liver parenchyma and image noise due to motion artifacts were improved in CS-eTHRIVE resulting in the improvement of SNR. So we believe that CS-eTHRIVE can contribute to shortening the acquisition time as well as compensate potential weakness in arterial phase breath holding for gadoxetic acid-enhanced MR imaging.Conclusion
CS-eTHRIVE sequence significantly reduced the acquisition time and TSM artifacts without degradation of image quality.Acknowledgements
No acknowledgement found.References
1. Kudo M, Matsui O, Izumi N, Iijima H, Kadoya M, Imai Y. Surveillance and diagnostic algorithm for hepatocellular carcinoma proposed by the Liver Cancer Study Group of Japan: 2014 update. Oncology 2014;87 Suppl 1:7-21.
2. Omata M, Cheng AL, Kokudo N, et al. Asia-Pacific clinical practice guidelines on the management of hepatocellular carcinoma: a 2017 update. Hepatology international 2017;11:317-70.
3. Goshima S, Noda Y, Kajita K, et al. Gadoxetic acid-enhanced high temporal-resolution hepatic arterial-phase imaging with view-sharing technique: Impact on the LI-RADS category. European journal of radiology 2017.
4. McClellan TR, Motosugi U, Middleton MS, et al. Intravenous Gadoxetate Acid Administration Reduces Breath-holding Capacity in the Hepatic Arterial Phase: A Multi-Center Randomized Placebo-controlled Trial. Radiology 2017;282:361-8.
5. Kaltenbach B, Bucher AM, Wichmann JL, et al. Dynamic Liver Magnetic Resonance Imaging in Free-Breathing: Feasibility of a Cartesian T1-Weighted Acquisition Technique With Compressed Sensing and Additional Self-Navigation Signal for Hard-Gated and Motion-Resolved Reconstruction. Investigative radiology 2017.
6. Weiss J, Notohamiprodjo M, Martirosian P, et al. Self-gated 4D-MRI of the liver: Initial clinical results of continuous multiphase imaging of hepatic enhancement. Journal of magnetic resonance imaging : JMRI 2017.
7. Yoon JH, Yu MH, Chang W, et al. Clinical Feasibility of Free-Breathing Dynamic T1-Weighted Imaging With Gadoxetic Acid-Enhanced Liver Magnetic Resonance Imaging Using a Combination of Variable Density Sampling and Compressed Sensing. Investigative radiology 2017.
Figures