2460
Pulmonary Perfusion MR Imaging with Ultra-Short TE: Comparison of Capability for Regional Perfusion Assessment and Postoperative Lung Function Prediction with Perfusion SPECT and/ or Conventional CT Methods1Division of Functional and Diagnostic Imaging Research, Department of Radiology, Kobe University Graduate School of Medicine, Kobe, Japan, 2Advanced Biomedical Imaging Research Center, Kobe University Graduate School of Medicine, Kobe, Japan, 3Toshiba Medical Systems Corporation, Otawara, Japan, 4Toshiba Medical Systems (China) Co., Ltd., Beijin, China, 5Division of Radiology, Department of Radiology, Kobe University Graduate School of Medicine, Kobe, Japan, 6Center for Radiology and Radiation Oncology, Kobe University Hospital, Kobe, Japan
Synopsis
Gadolinium-based blood volume (Gd-based BV) map generated between unenhanced and contrast-enhanced UTE-MRIs may have a potential for regional perfusion assessment like lung perfused BV map on dual-energy CT in patients with pulmonary diseases. We hypothesized that Gd-based BV map has a potential to regional perfusion assessment and postoperative lung function prediction as well as perfusion SPECT and/ or conventional CT methods in NSCLC patients. The purpose of this study was to directly compare the capability of Gd-based BV map for regional perfusion assessment and/ or postoperative lung function prediction in NSCLC patients with perfusion SPECT and conventional CT methods.
Introduction
Despite advances in radiation therapy and chemotherapy, surgery is currently considered the best curative option for stage I, II or IIIA non-small cell lung cancer (NSCLC) patients. In general, many potentially resectable tumors occur in individuals with abnormal pulmonary functions, thus increasing operative risk. Therefore, a few guidelines and/ or algorithms are suggested as useful for prediction of postoperative lung function in candidates for surgical treatment to NSCLC. Since 2013, pulmonary MR imaging with ultrashort TE (UTE-MRI) has been suggested as having a potential to demonstrate lung structures and morphological assessment as well as CT in last several years (1-3). However, there were no reports assessed the potential of pulmonary MR imaging with UTE for pulmonary functional assessment at 3T systems. Recently, we can generate gadolinium-based blood volume (Gd-based BV) map by subtraction between unenhanced and contrast-enhanced UTE-MRIs may have a potential for regional perfusion assessment like lung perfused blood volume map on dual-energy CT in patients with pulmonary diseases. Moreover, no one compare its’ potential for prediction of postoperative lung function than other modalities in NSCLC patients. We hypothesized that Gd-based BV map from unenhanced and contrast-enhanced UTE-MRIs has a potential to regional perfusion assessment and postoperative lung function prediction as well as perfusion SPECT and/ or conventional CT methods in NSCLC patients. The purpose of this study was to directly compare the capability of Gd-based BV map generated from unenhanced and contrast-enhanced UTE-MRIs for regional perfusion assessment and/ or postoperative lung function prediction in NSCLC patients with perfusion SPECT and conventional CT methods.Materials and Methods
Twenty-nine consecutive NSCLC patients (16 males and 13 females: mean age ± standard deviation [SD]: 65.7 ± 11.1 years), who were candidates for surgical treatment, underwent unenhanced and contrast-enhanced UTE-MRIs, thin-section CT, perfusion SPECT, and measurements of FEV1% before and after lung resection. All UTE-MRIs were examined by a 3T MR system (Vantage Titan 3T, Toshiba) by respiratory-gated 3D radial UTE pulse sequence (TR 4.0 ms/ TE 110 μs, flip angle 5 degree, 1×1×1 mm3 voxel size). On Gd-based BV map and perfusion SPECT, each regional perfusion rate within the resected lobe was determined as contrast enhancement and radioisotope uptake ratios between resected lobe and total lung. Then, postoperative FEV1% (poFEV1%) was predicted from Gd-based BV map (poFEV1%UTE-MRI) and perfusion SPECT (poFEV1%Perfusion SPECT) were assessed from regional perfusion rate within total and resected lungs. Quantitatively and qualitatively CTs were predicted poFEV1%s (poFEV1%Quantitative CT and poFEV1%Qualitative CT) from the functional lung volumes determined by commercially available software and numbers of segment between resected and total lung. To determine the capability of Gd-based BV map for regional perfusion assessment, regional perfusion rate of Gd-based BV map was statistically correlated with that of perfusion SPECT. To determine the capability for prediction of postoperative lung function among four methods, each predicted poFEV1% was correlated with actual poFEV1%. Finally, the limits of agreement (mean±1.96´standard deviation) between actual and each predicted poFEV1%s were also evaluated by Bland-Altman analysis. A p value less than 0.05was considered as significant in each statistical analysis.Results
Representative case is shown in Figure 1. Regional perfusion rate of Gd-based BV map had significant and excellent correlations with that of perfusion SPECT (r=0.90, p<0.0001). Correlation and the limits of agreement between each poFEV1% and actual poFEV1% are shown in Figure 2. There are significant and excellent correlations between actual poFEV1% and each poFEV1% (0.74±0.86, p<0.0001). The limits of agreement of Gd-based BV map (4.3±12.7%) were smaller than that of qualitatively assessed CT (5.1±13.9%), and almost equal to that of quantitatively assessed CT (3.5±10.8%) and perfusion SPECT (4.2±14.5%).Conclusion
Gd-based BV map generated between unenhanced and contrast-enhanced pulmonary MR imaging with UTE has similar or slightly better capability for postoperative lung function prediction in NSCLC patients, when compared with quantitatively and qualitatively assessed CT and perfusion SPECT.Acknowledgements
This study was supported by Toshiba Medical Systems Corporation.References
- Johnson KM, Fain SB, Schiebler ML, Nagle S. Magn Reson Med. 2013; 70: 1241-1250.
- Ohno Y, Koyama H, Yoshikawa T, et al. J Magn Reson Imaging. 2016; 43: 512-532.
- Ohno Y, Koyama H, Yoshikawa T, et al. Radiology. 2017; 284: 562-573.
Figures

Figure 1. 62-year old male with invasive adenocarcinoma with mild COPD (L to R: Thin-section MPR image of CT, quantitatively assessed thin-section MPR image, axial and coronal perfusion SPECT, source imae of unenhanced UTE-MRI and Gd-based BV map generated from unenhanced and contrast-enhanced UTEs).
All methods clearly demonstrate lung cancer (arrow) in the left upper lobe. On quantitatively assessed CT, low attenuation areas equal to or less than -950HU were demonstrated as blue. On quantitatively and qualitatively assessed CT, pulmonary emphysema was shown as heterogeneous but upper lung field dominant distributions in both lungs except lung cancer (arrow) On the other hand, perfusion SPECT shows homogeneous uptakes in both lung except lung cancer (arrow). Gd-based BV map generated between unenhanced and contrast-enhanced UTE-MRIs shows heterogeneous enhancement within both lung due to pulmonary emphysema except lung cancer (arrow).
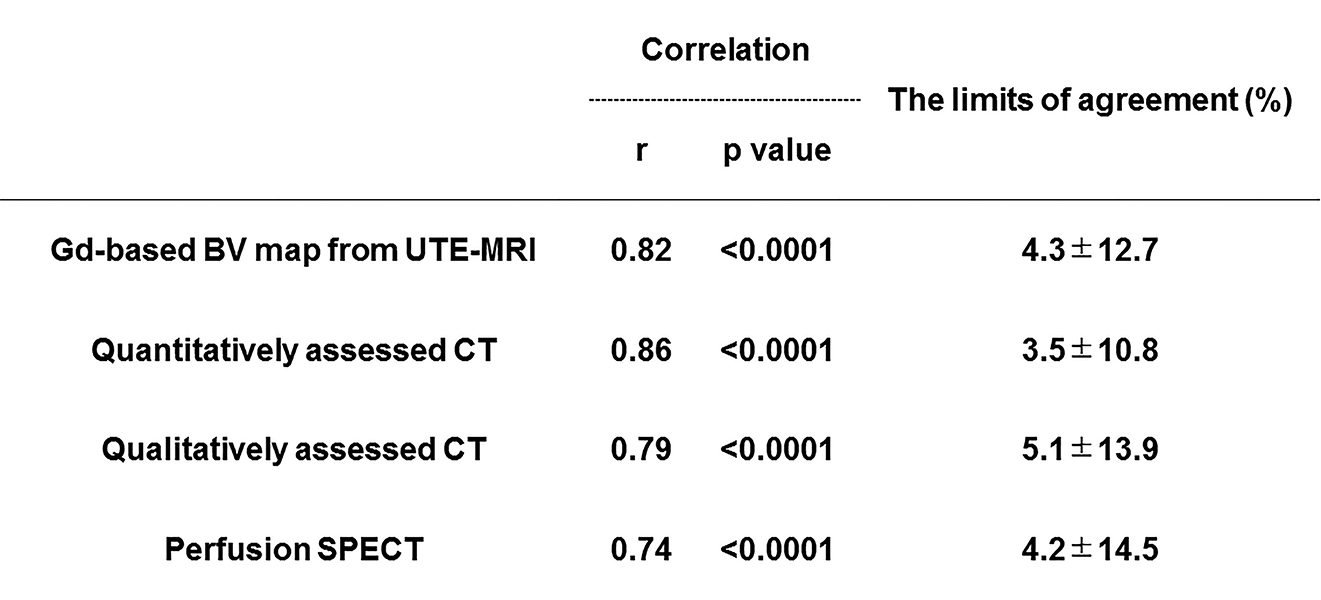
Figure 2. Correlation and the limits of agreement between each poFEV1% and actual poFEV1%.
There are significant and excellent correlations between actual poFEV1% and each poFEV1% (0.74≤r≤0.86, p<0.0001). The limits of agreement of Gd-based BV map (4.3±12.7%) were smaller than that of qualitatively assessed CT (5.1±13.9%), and almost equal to that of quantitatively assessed CT (3.5±10.8%) and perfusion SPECT (4.2±14.5%).