2451
Usefulness of morphological characteristics for the differentiation of benign from malignant peripheral solitary pulmonary lesions using MR T1-weighted 3D Star VIBE1Department of Radiology, Affiliated Hospital of Shaanxi University of traditional Chinese Medicine, XianYang, China, 2Siemens Healthcare, Scientific marketing, China, Shanhai, China, 3Shaanxi University of traditional Chinese Medicine, XianYang, China
Synopsis
Can MR T1-weighted 3D Star VIBE alternate the MSCT in morphological features of the peripheral solid pulmonary lesions?
Background and purpose
The mortality of lung cancer is high, and the differentiation of benign and malignant peripheral solid pulmonary lesions(PSPLs)is very important. High resolution CT is the most commonly used radiology methods for differentiating the benign and malignant PSPLs. While it is limited to children、pregnant women and disorders requiring repeated examinations over prolonged periods because of its radiation exposure. T1-weighted 3D Star VIBE sequence obtaining scan under free breathing can also provide high-resolution imaging (1.2mm), and can also compensate for breathing, heart and large blood vessel pulsation and other motion artifacts. In this study, we compared morphological characteristics of PSPLs obtained from T1-weighted 3D Star VIBE sequence and MSCT respectively,and evaluated initially capability of T1 Star VIBE sequence for distinguishing malignant PSPLs from benign.Methods
The institutional review board approved this study, and written informed consent was obtained from each patient. Chest spiral CT examination and MR (3 T MR scanner) imaging with T1 Star VIBE were used to examine 47 patients; 30 males and 17 females (mean age, 64.1 years old; age range, 48–83 years). Most of lesions were using transthoracic needle biopsy, a few patients were completely surgically resected. The benign and malignant PSPLs were finally identified by pathology results. Two radiologists observed the morphological signs independently (margins, contour, internal characteristics, visceral pleural and mediastinal lymph node) for MR and CT images. The MR images scanned first, and followed by CT. The display of morphological characteristics of MR and CT was divided into either “visible” or “invisible”. The kappa test was used to compare the morphological characteristics display capability between the two methods,and k value was used to compare inter-method agreement. The ROC curve was used to analyze the capabilities of morphological characteristics in distinguishing malignant PSPLs from benign one.Results
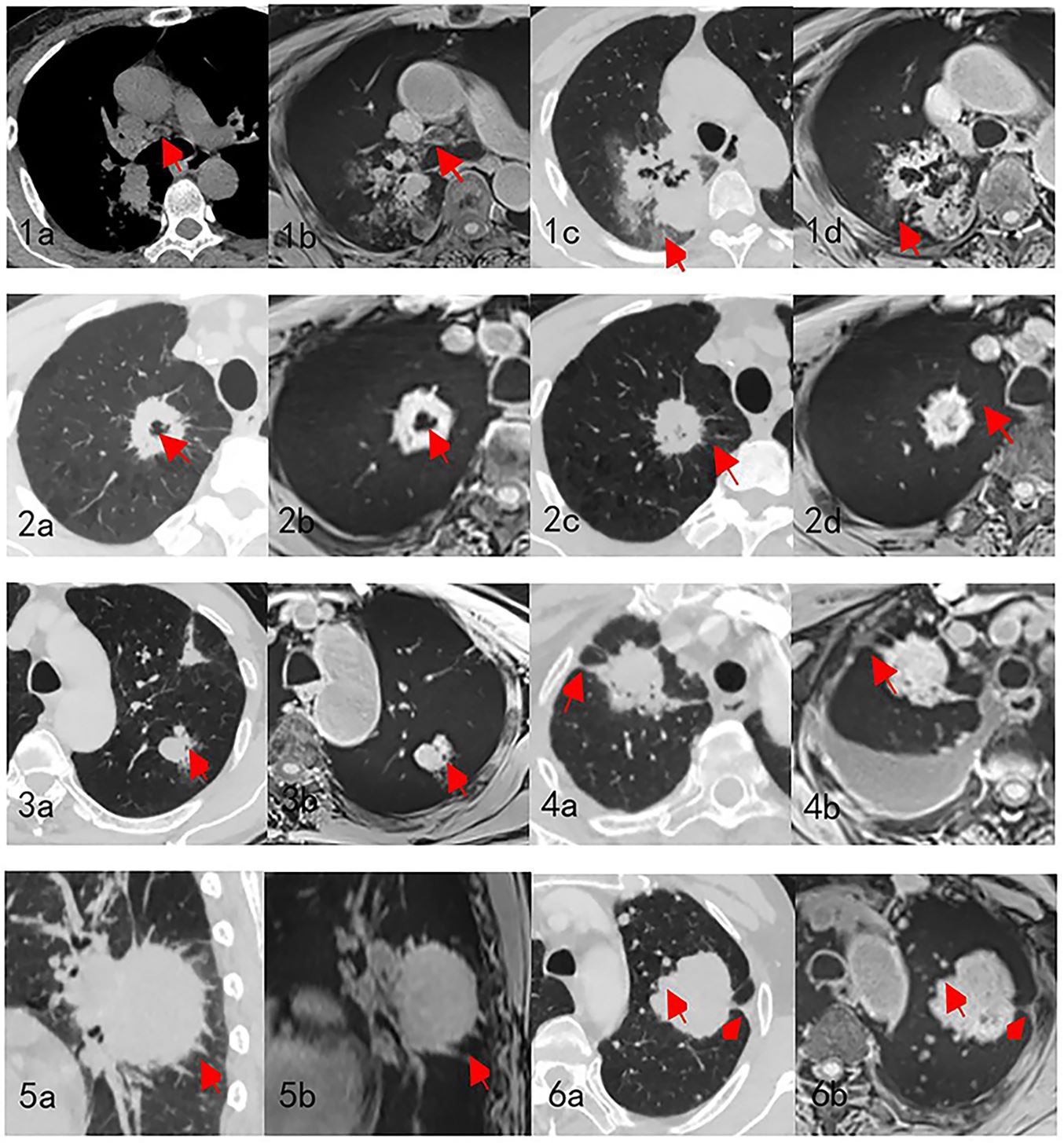
Totally 47 PSPLs were observed, and the average maximum diameter was about 3.94 + 1.91cm. Inter-method agreement was excellent. No significant differences were found in displaying morphological characteristics in both imaging obtained from MR T1 Star VIBE and CT, including internal characteristics, peripheral structure and visceral pleural. However, the morphological characteristics of mediastinal lymph node enlargement and lobulation were visible in both MR T1 Star VIBE (mediastinal lymph node enlargement: p=0.036, lobulation: p=0.033) and CT (mediastinal lymph node enlargement: p=0.009, lobulation: p=0.005). It found that Lobular shape and mediastinal lymph node enlargement were more easily to be found in malignant lesion. According to the ROC analysis, the area under curve(AUC), sensitivity and specificity are 0.794, 0.727, 0.778, respectively for MR T1 Star VIBE, and 0.836, 0.909 and 0.722 for CT.The MR T1 Star VIBE and CT map were seen in Figure1.conclusion
Among these morphological features, only mediastinal lymph node enlargement and lobulation features can be used to distinguish between the benign and malignant PSPLs. The diagnostic efficacy of MR T1 Star VIBE was slightly lower than CT. Although it cannot completely replace the high resolution of CT, it can be used as an alternative method to distinguish malignant PSPLs from benign without radiation.Acknowledgements
NoReferences
1.Schaefer, J. F., Vollmar, J., Wiskirchen, J., Erdtmann, B., D, V. R., Vonthein, R., . . . Seemann, M. D. (2006). Differentiation between malignant and benign solitary pulmonary nodules with proton density weighted and ECG-gated magnetic resonance imaging. European Journal of Medical Research, 11(12), 527-533.
2.Seemann, M. D., Staebler, A., Beinert, T., Dienemann, H., Obst, B., Matzko, M., . . . Reiser, M. F. (1999). Usefulness of morphological characteristics for the differentiation of benign from malignant solitary pulmonary lesions using HRCT. European Radiology, 9(3), 409-417.
3.Kuriyama, K., Tateishi, R., Doi, O., Kodama, K., Tatsuta, M., Matsuda, M., . . . Fujita, M. (1987). CT-pathologic correlation in small peripheral lung cancers. Ajr American Journal of Roentgenology, 149(6), 1139-1143.
Figures