2432
Apparent Diffusion Coefficient as a Quantitive Imaging Biomarker for Prediction of Immunohistochemical Receptor Status, Proliferation Rate and Molecular Subtypes of Breast Cancer1Radiology, Memorial Sloan Kettering Cancer Center, New York, NY, United States, 2Medical Physics, Memorial Sloan Kettering Cancer Center, New York, NY, United States, 3Medical University of Vienna, Vienna, Austria
Synopsis
Molecular subtype classification of breast tumor is of paramount importance in determining aggressiveness and prognosis. The ability to use diffusion weighted imaging (DWI) for the prediction of molecular subtypes may improve management in breast cancer. In this study, two radiologists retrospectively evaluated different metrics on apparent diffusion coefficient maps of 107 patients with invasive breast cancer. ER and PR positive lesions had lower ADC values while HER2 positive and high-proliferating had higher values. Luminal cancers had lower ADC values than other subtypes, thus DWI may be used to predict tumor subtype in breast cancer.
Introduction
Magnetic resonance imaging (MRI) is an essential tool for the diagnosis and staging of breast cancer (1, 2). To improve limitations on specificity, diffusion weighted imaging (DWI) has emerged as a robust MRI parameter. DWI measures the random motion of water molecules, which can be quantified by the apparent diffusion coefficient (ADC) (3-7). Immunohistochemical (IHC) receptor status, i.e presence of estrogen receptor (ER), progesterone receptor (PR), human epidermal growth factor receptor 2 (HER2) and proliferation rate (Ki-67) are major prognostic factors and are predictive of response to neoadjuvant treatment. Based on IHC-surrogates, molecular subtypes can be defined (8, 9). However, to date the receptor status and proliferation rate has to be obtained by tissue sampling and up to 20% of patients show disagreement between biopsy and surgical specimen (10-12). ADC has been investigated for predicting IHC status but results are divergent (12-21). Therefore, the aim of the study was to evaluate whether different ADC metrics can be used for prediction of IHC status and molecular subtype in breast cancer.Material and Methods
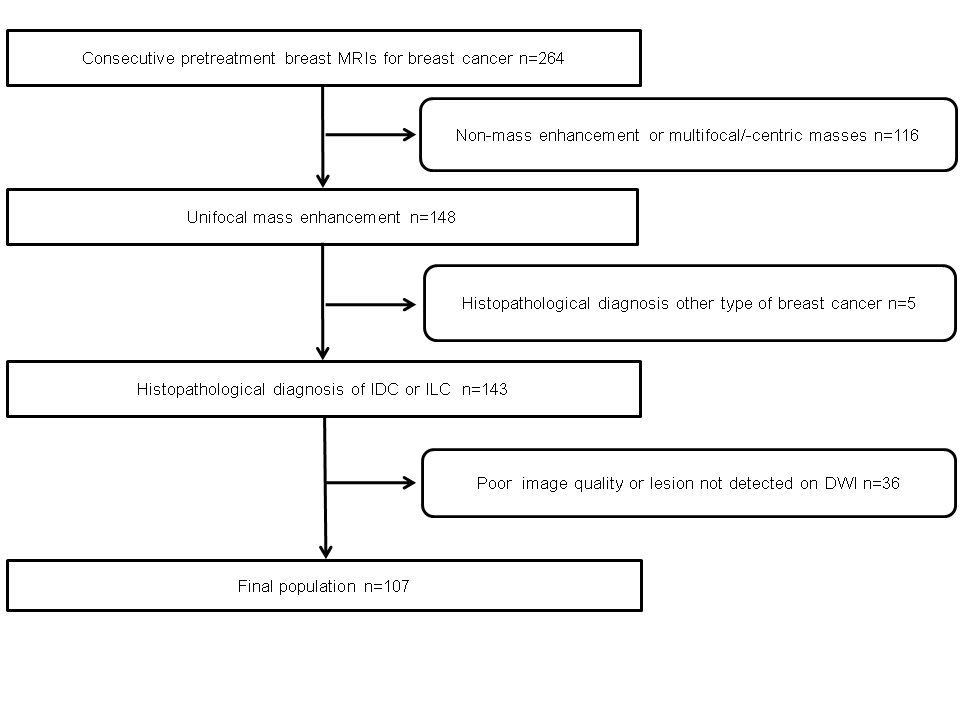
The Institution Review Board approved this retrospective study, which selected patients who underwent MRI of the breast with DWI between 12/2010 and 02/2014 and fulfilled the following inclusion criteria: histopathologically verified invasive breast cancer, 18 years or older; not pregnant or breastfeeding; no previous treatment; and no contraindications for MRI or contrast agents. The exclusion criteria were 1) non-mass enhancement or multiple masses, 2) Other types of cancer than invasive ductal carcinoma (IDC) or invasive lobular carcinoma (ILC), 3) poor image quality or lesion not detected on DWI. Overall, 107 patients were included in the study (Figure 1).
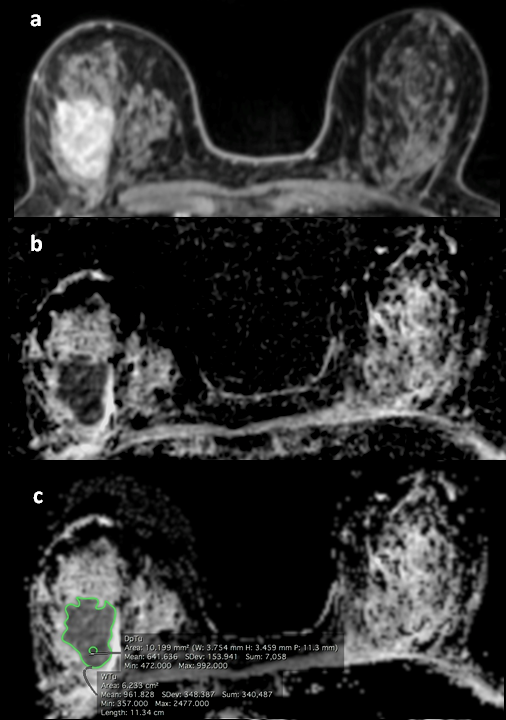
MRI studies were independently evaluated by two board-certified radiologists with 6 (reader 1) and 12 years (reader 2) of experience in breast MR imaging. The tumors were identified on high-b-value (850 s/mm2) using DCE-MR images as anatomical guidance. The radiologists chose the slice with the greatest representative portion of the tumor and drew one 2-dimensional region of interest (ROI) on the whole tumor (WTu) on ADC maps, and another 2-dimensional ROI on the darkest part (Dp) of the tumor (Figure 2). The minimum, mean and maximum ADC values of both the WTu and Dp were compared with histopathology, grade, ER, PR, HER 2 and Ki-67 status and molecular subtype.
Results
ER, PR and HER2 status was available in all 107 patients, and Ki-67 in 87. ER, PR positive tumors had lower ADC values, while HER2 positive and KI-67 high-proliferating lesions had higher values. Differentiation among molecular subtypes were statistically significant for both readers. Luminal tumors had lower ADC values while HER2-enriched tumors had the highest. Differentiation between luminal tumors and other subtypes were possible for Dp mean, Dp minimum, WTu mean, WTu minimum and WTu maximum measurements for both readers (p<0.0001). The areas under the curve were higher for measurements of the WTu mean (0.685 for both readers) and WTu maximum (0.606 for reader 1 and 0.627 for reader 2). Comparing luminal A tumors, that had the lowest values, with all other subtypes combined, we found that all measurements were statistically significant for both readers (p<0.0001). The areas under the curve were also higher for measurements of the WTu mean (0.647 for reader 1 and 0.685 for reader 2) and WTu maximum (0.698 for reader 1 and 0.659 for reader 2).Discussion
The ADC values were lower in ER and PR positive and higher in HER2 positive and high-proliferating tumors. ADC values were significantly different among molecular subtypes and could differentiate luminal tumors from all other subtypes. The diagnosis of luminal A lesions is of paramount clinical importance since they might benefit less from neo- and adjuvant chemotherapy. The increased cellularity seen in most breast cancers causes a restriction in the movement of water particles and reduces the ADC values (13). Therefore, high-proliferating tumors are expected to have lower ADC than low-proliferating tumors. On the other hand, a greater amount of extracellular fluid due to an increased neovacularity with greater permeability in a tumor can increase ADC values, a phenomenon which has been observed in HER2 positive lesions (16, 21). In contrast, ER positive tumors, tend to have less neovascularity and therefore lower ADC values, as observed in our study (13, 16).Conclusion
In conclusion, ADC measurements have the potential to non-invasively determine IHC status and differentiate molecular subtypes.Acknowledgements
No acknowledgement found.References
1. Mann RM, Balleyguier C, Baltzer PA, Bick U, Colin C, Cornford E, et al. Breast MRI: EUSOBI recommendations for women's information. European radiology. 2015;25(12):3669-78. 2. Sardanelli F, Boetes C, Borisch B, Decker T, Federico M, Gilbert FJ, et al. Magnetic resonance imaging of the breast: recommendations from the EUSOMA working group. European journal of cancer. 2010;46(8):1296-316. 3. Partridge SC, DeMartini WB, Kurland BF, Eby PR, White SW, Lehman CD. Quantitative diffusion-weighted imaging as an adjunct to conventional breast MRI for improved positive predictive value. AJR American journal of roentgenology. 2009;193(6):1716-22. 4. Pinker K, Helbich TH, Morris EA. The potential of multiparametric MRI of the breast. The British journal of radiology. 2017;90(1069):20160715. 5. Tan SL, Rahmat K, Rozalli FI, Mohd-Shah MN, Aziz YF, Yip CH, et al. Differentiation between benign and malignant breast lesions using quantitative diffusion-weighted sequence on 3 T MRI. Clinical radiology. 2014;69(1):63-71. 6. Cheeney S, Rahbar H, Dontchos BN, Javid SH, Rendi MH, Partridge SC. Apparent diffusion coefficient values may help predict which MRI-detected high-risk breast lesions will upgrade at surgical excision. Journal of magnetic resonance imaging : JMRI. 2017. 7. Bickel H, Pinker K, Polanec S, Magometschnigg H, Wengert G, Spick C, et al. Diffusion-weighted imaging of breast lesions: Region-of-interest placement and different ADC parameters influence apparent diffusion coefficient values. European radiology. 2017;27(5):1883-92. 8. Cipolla V, Santucci D, Guerrieri D, Drudi FM, Meggiorini ML, de Felice C. Correlation between 3T apparent diffusion coefficient values and grading of invasive breast carcinoma. European journal of radiology. 2014;83(12):2144-50. 9. Baba S, Isoda T, Maruoka Y, Kitamura Y, Sasaki M, Yoshida T, et al. Diagnostic and prognostic value of pretreatment SUV in 18F-FDG/PET in breast cancer: comparison with apparent diffusion coefficient from diffusion-weighted MR imaging. J Nucl Med. 2014;55(5):736-42. 10. Mann GB, Fahey VD, Feleppa F, Buchanan MR. Reliance on hormone receptor assays of surgical specimens may compromise outcome in patients with breast cancer. J Clin Oncol. 2005;23(22):5148-54. 11. Burge CN, Chang HR, Apple SK. Do the histologic features and results of breast cancer biomarker studies differ between core biopsy and surgical excision specimens? Breast. 2006;15(2):167-72. 12. Martincich L, Deantoni V, Bertotto I, Redana S, Kubatzki F, Sarotto I, et al. Correlations between diffusion-weighted imaging and breast cancer biomarkers. Eur Radiol. 2012;22(7):1519-28. 13. Choi SY, Chang YW, Park HJ, Kim HJ, Hong SS, Seo DY. Correlation of the apparent diffusion coefficiency values on diffusion-weighted imaging with prognostic factors for breast cancer. The British journal of radiology. 2012;85(1016):e474-9. 14. Guvenc I, Akay S, Ince S, Yildiz R, Kilbas Z, Oysul FG, et al. Apparent diffusion coefficient value in invasive ductal carcinoma at 3.0 Tesla: is it correlated with prognostic factors? The British journal of radiology. 2016;89(1060):20150614. 15. Jeh SK, Kim SH, Kim HS, Kang BJ, Jeong SH, Yim HW, et al. Correlation of the apparent diffusion coefficient value and dynamic magnetic resonance imaging findings with prognostic factors in invasive ductal carcinoma. Journal of magnetic resonance imaging : JMRI. 2011;33(1):102-9. 16. Karan B, Pourbagher A, Torun N. Diffusion-weighted imaging and (18) F-fluorodeoxyglucose positron emission tomography/computed tomography in breast cancer: Correlation of the apparent diffusion coefficient and maximum standardized uptake values with prognostic factors. Journal of magnetic resonance imaging : JMRI. 2016;43(6):1434-44. 17. Kim SH, Cha ES, Kim HS, Kang BJ, Choi JJ, Jung JH, et al. Diffusion-weighted imaging of breast cancer: correlation of the apparent diffusion coefficient value with prognostic factors. Journal of magnetic resonance imaging : JMRI. 2009;30(3):615-20. 18. Kitajima K, Yamano T, Fukushima K, Miyoshi Y, Hirota S, Kawanaka Y, et al. Correlation of the SUVmax of FDG-PET and ADC values of diffusion-weighted MR imaging with pathologic prognostic factors in breast carcinoma. European journal of radiology. 2016;85(5):943-9. 19. Lee HS, Kim SH, Kang BJ, Baek JE, Song BJ. Perfusion Parameters in Dynamic Contrast-enhanced MRI and Apparent Diffusion Coefficient Value in Diffusion-weighted MRI:: Association with Prognostic Factors in Breast Cancer. Academic radiology. 2016;23(4):446-56. 20. Nakajo M, Kajiya Y, Kaneko T, Kaneko Y, Takasaki T, Tani A, et al. FDG PET/CT and diffusion-weighted imaging for breast cancer: prognostic value of maximum standardized uptake values and apparent diffusion coefficient values of the primary lesion. Eur J Nucl Med Mol Imaging. 2010;37(11):2011-20. 21. Park SH, Choi HY, Hahn SY. Correlations between apparent diffusion coefficient values of invasive ductal carcinoma and pathologic factors on diffusion-weighted MRI at 3.0 Tesla. Journal of magnetic resonance imaging : JMRI. 2015;41(1):175-82.Figures