2423
Application of multiple b-value diffusion weighted imaging in diagnosing ductal carcinoma in situ1Radiology, The First affiliated hospital of Dalian Medical University, Dalian, China, 2Radiology, The Second affiliated hospital of Dalian Medical University, Dalian, China, 3GE healthcare, China, Beijing, China
Synopsis
Multiple b-value diffusion weighted imaging (DWI) provides quantitative measurement of ADCslow for cellularity and ADCfast and ffast for vascularity. It is helpful for the differentiation between benign and malignant breast lesions. This study concerned perfusion as well as diffusion information in normal breast tissues and breast lesions from intravoxel incoherent motion (IVIM) imaging based on the biexponential analysis of multiple b-value DWI and then compared these parameters to ADC obtained with monoexponential analysis on the diagnosis of different grades of ductal carcinoma in situ (DCIS).
Purpose
To explore the feasibility of multiple b-value DWI for differentiation of low-grade and intermediate/high-grade DCIS.Methods
In this prospective study, a total of 26 female patients (MR grade: BI-RADS 4) were enrolled and informed consent was acquired from each patient. Specifically, group 1 included 12 patients with low-grade DCIS, and group 2 included 5 patients with intermediate-grade DCIS and 9 patients with high-grade DCIS. Multiple b-value DWI (18 b value) were acquired. DWI parameters (ADCstandard, ADCslow, ADCfast and ffast) of lesions and contralateral fibroglandular tissue (FGT) were analyzed. The parameters were compared between two groups and the diagnostic performance based on different parameters was quantified with ROC curve.
Results
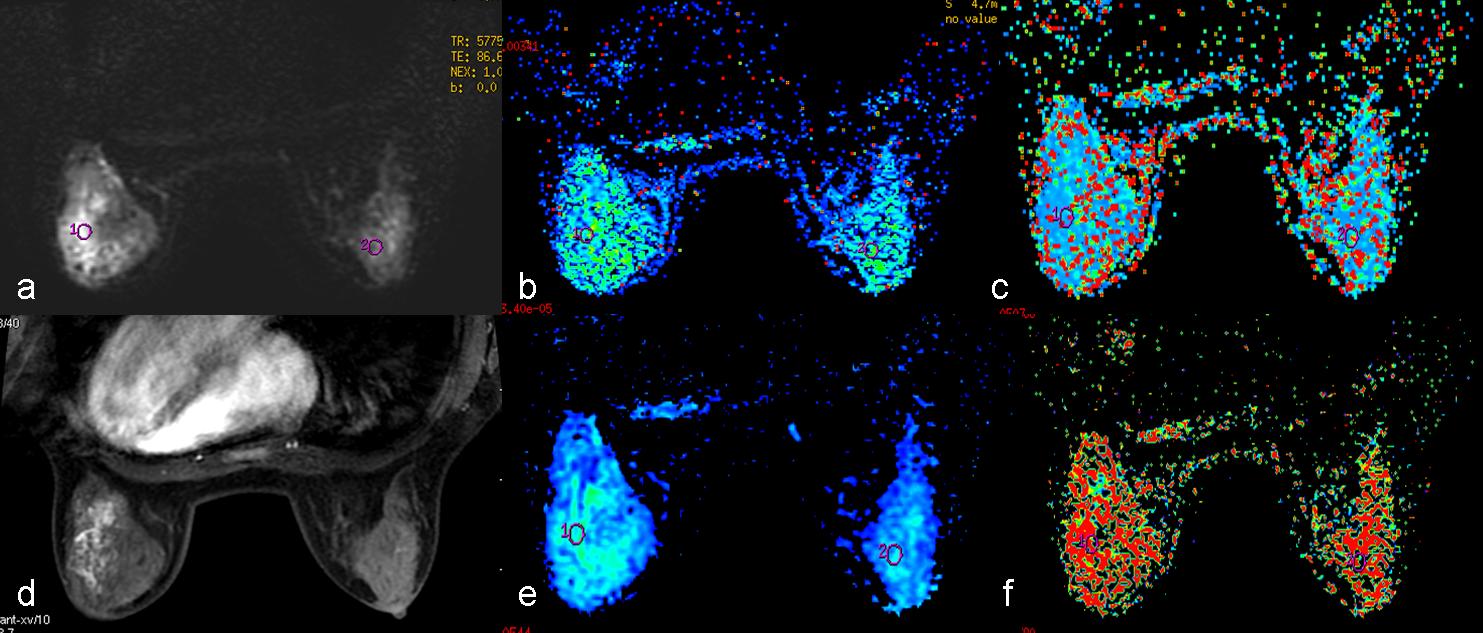
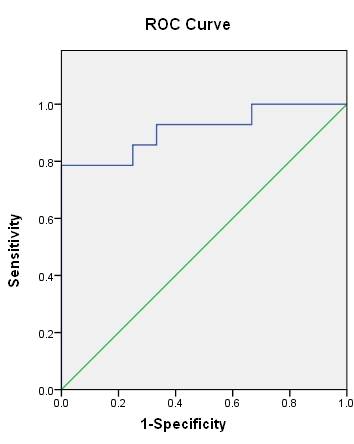
There was no significant difference in age and maximal lesion diameter between two groups (p=0.257, 0.056). The ADCstandard and ADCslow of low-grade DCIS lesions were significantly higher than those of intermediate/high-grade lesions (p=0.008, 0.000). ADCslow and ADCfast were statistically significant between low-grade DCIS lesions and FGT (p=0.041, 0.036), while ADCstandard and ffast were not (p=0.207, 0.473). All parameters showed significant differences between intermediate/high-grade lesions and FGT (p=0.000, 0.000, 0.009, 0.033) (Fig1). The highest area under the curve (AUC) was acquired by combining ADCslow and ADCstandard with an optimal threshold of 0.266×10-3mm2 (Fig2).
Discussion and Conclusion
DCIS lesions usually do not become invasive, while patients diagnosed with DCIS are usually treated as those diagnosed with invasive carcinoma[1]. New biomarkers should be introduced for accurate prediction of the grade and outcome of patients diagnosed with DCIS and thereby reduce unnecessary use of extensive surgery[2]. In comparison to DWI with monoexponential fit, multiple b-value DWI provides quantitative measurement of ADCslow for cellularity and ffast for vascularity[3,4]. This study suggests that the parameters derived from multiple b-value DWI are useful in distinguishing low-grade DCIS from intermediate/high-grade DCIS. The highest diagnostic performance can be achieved by combing ADCslow and ADCstandard for the differentiation of different grades of DCIS. Consequently, patients with DCIS can be spared from mastectomy or axillary lymph node dissection.Acknowledgements
This work has not received any funding.References
[1] Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015. CA Cancer J Clin. 2016,66(2): 115-132.
[2] Iima M, Le Bihan D, Okumura R,et al. Apparent diffusion coefficient as an MR imaging biomarker of low- risk ductal carcinoma in situ: a pilot study. Radiology. 2011, 260(2):364-72.
[3] Lee YJ, Kim SH, Kang BJ, et al. Intravoxel incoherent motion (IVIM)-derived parameters in diffusion weighted MRI: Associations with prognostic factors in invasive ductal carcinoma. J Magn Reson Imaging.
2017,45(5): 1394-1406.
[4] Kim Y J, Ko K, Kim D H, et al. Intravoxel incoherent motion diffusion-weighted MR imaging of breast cancer: Association with histopathological features and subtypes. Br J Radiol. 2016, 89(1063): 20160140.
Figures