2369
Assessing cue-induced brain response in heroin-dependents treated by methadone maintenance and protracted abstinence measures1Department of Radiology, Tangdu Hospital, The Fourth Military Medical University, Xi'an, China, 2radiology department of Tangdu hospital, The Fourth Military Medical University, Xi’an, China, 3Radiology department of Tangdu hospital, The Fourth Military Medical University, Xi’an, China
Synopsis
Our research aimed to compare PA with MMT,to reveal which abstinence way is better to recover the brain function in heroin-dependent individuals.24 heroin-dependent patients under PA ,19 heroin-dependent patients under MMT and 20 healthy volunteers were recruited. The functional images were acquired by using a spin-echo EPI. In the last part of this study, we proved PA group is closer to healthy group.This study showed that PA is more advantageous than MMT to reduce heroin addiction in drug cue-reactivity.
Purpose
Heroin addiction (HA) has been associated with impairments in a broad range of cognitive functions. Craving is an important factor in heroin addiction, and cue-induced craving is an especially powerful form of this construct. Task-based studies have demonstrated that a certain part of default mode network such as medial prefrontal cortex, is closely associated with drug craving and relapse [1,2]. An event-related cue-reactivity paradigm was employed. For heroin-dependent, protracted abstinence (PA) and methadone maintenance therapy (MMT) are two common therapeutic methods in heroin dependence, and both of them suppress subjective feeling of drug craving. This study was combined fMRI and a drug cue-reactivity task,aimed to shed light on the two therapeutic methods which one is better and what is the relationship between drug cue-reactivity and the two different therapeutic methods , in order to recover and improve brain function in clinical.
Materials and Methods
We applied 24 heroin-dependent males with at least 6 months of PA, 19 heroin-dependent male patients stabilized on MMT for at least 6 months and 20 demographically matched healthy controls completed an event-related fMRI task including heroin-related and neutral cues. All subjects were performed the heroin cue-reactivity task during fMRI. Subjects inclusion criteria included: meeting the diagnostic criteria of DSM-IV for heroin addiction; adult male and right-handed; normal control subjects had no current or lifetime history of any DSM-IV substance use or psychiatric disorder.
A routine structure T2WI image was conducted to exclude any gross cerebral abnormality. The functional component of the image was acquired by using a spin-echo EPI (echo planar imaging): For each volume,32 axial slices covering the whole brain :repetition time = 2000 milliseconds, field of view = 256×256 mm2, slice thickness = 4 mm, spatial resolution = 4×4×4 mm3 and so on. To facilitate co-registration of the fMRI data in standard space, a 166-slice high-resolution fast spoiled gradient-echo 3D T1-weighted image was also collected with the following parameters Data Processing Assistant for fMRI (DPARSF) within Matlab software was used in the data preprocessing process of the functional images. The fMRI data analysis was conducted with SPM8 software .The functional scans were realigned to the first image with the volume of 150, and head motion correction was processed to get the corresponding mean functional image. The images were normalized with the voxel size of 3 × 3 × 3 mm by using an EPI template and spatially smoothed with a FWHM of 8 mm.
Results
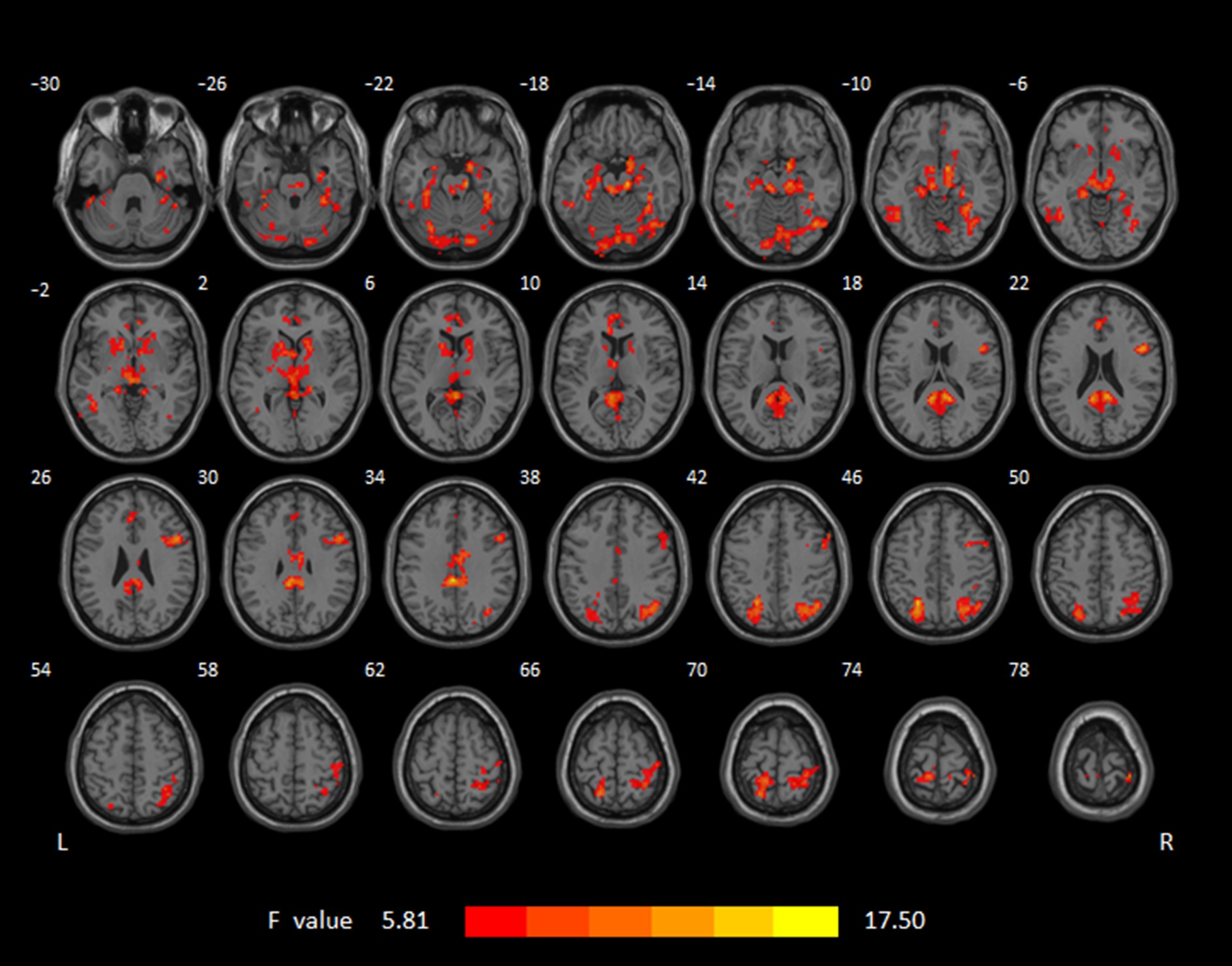
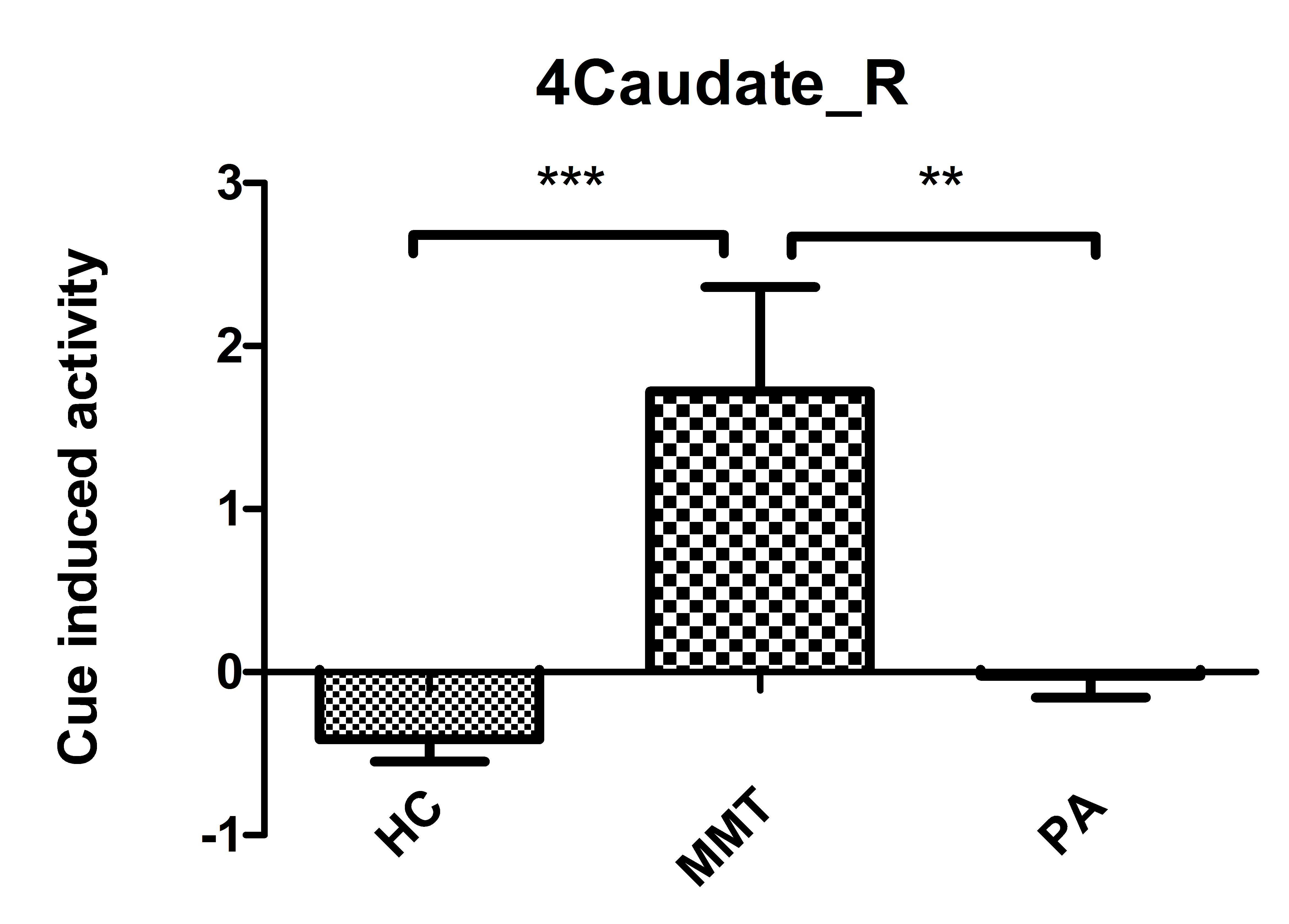
Under the condition of heroin-related > neutral cues, MMT group, PA group and healthy group in drug cues have a statistically significant difference between the response in 21 brain areas(P<0.05), the significantly increased brain responses during the processing of heroin-related cues concentrated expression in mesencephalic limbic dpamine system (such as caudate, midbrain, thalamus, hippocampal gyrus), prefrontal regions (DLPFC), visuospatial-attention regions (fusiform Gyrus, inferior parietal lobule, superior parietal lobule, occipital area)and cerebellum. Post hoc analysis showed that MMT group were significantly enhanced in cue-reactivity in the above brain regions than the PA and healthy group; compared with healthy group, PA group was no statistical differences in the brain regions. Brain areas in MMT group and PA group which have no differences in cue-reactivity intensity and no significant correlation with craving changes,but the cue induced activity of PA group closes to healthy group. This study showed that in the same phase cue-reactivity in PA group is lower than in MMT group, and drug cue-reactivity of PA group is closer to healthy group than MMT group.
Discussion and Conclusion
In previous reports, little research was compared PA with MMT, and little known which therapeutic method is help patients to get good withdrawal effect[3]. Here, we obtained new results about this. We know that the four classical neural circuits associated with addiction include reward circuit, motivation/drive circuit, memory and learning circuit and cognitive control circuit [4]. In our results, these brain regions are related to mesolimbic dopamine system (reward), Visual-spatial attention system (craving) and Prefrontal system (inhibitory control), which are important to research drug addiction[5].All of the results indicated that heroin-related cues can induce enhanced salience attribution among the heroin-dependent patients under PA and MMT. Our research has revealed that PA is better than MMT in heroin abstinence and PA is more conducive to the improvement and recovery of brain function in heroin addicts. So compared with MMT, PA is more advantageous to reduce heroin addiction in drug cue-reactivity, which can reduce salience value in drug cue for heroin addiction, in order to reduce the relapse susceptibility of the heroin addicts.
Acknowledgements
This work was supported by the grants from the National Natural Science Foundation of China (Nos. 30870685, 81071142,81071143 and 81671661) and the Development Project of Science and Technology of Shaanxi Province. We thank Xinhai Wu for contributions to the recruitment of heroin subjects.References
1. Seo, D, et al. Disrupted ventromedial prefrontal function, alcohol craving, and subsequent relapse risk. JAMA Psychiatry, 2013,70(7):727-39.
2. Janes, A.C, et al. Brain reactivity to smoking cues prior to smoking cessation predicts ability to maintain tobacco abstinence. Biol Psychiatry,2010,67(8):722-9.
3.Qiang Li, Yarong Wang, Yi Zhang et al. Craving correlates with mesolimbic responses to heroin-related cues in short-term abstinence from heroin: An event-related fMRI study. Brain Res.2012,21(8):1469:63-72.
4.Volkow, N. D., Wang, G. J., Fowler, J. S., Tomasi, D., & Telang, F. Addiction: beyond dopamine reward circuitry. Proc Natl Acad Sci U S A, 2011,108(37), 15037-15042, doi:10.1073/pnas.1010654108.
5. Volkow ND, Li T-K .Drug addiction: the neurobiology of behaviour gone awry. Nat Rev Neurosci,2004, 5:963–970.
Figures