2366
Acute stress modulates cigarette cue-evoked neural activation: A neuropharmacological investigation among non-treatment-seeking cigarette smokersEric Woodcock1, Vaibhav Diwadkar2, Jeffrey Stanley2, Dalal Khatib2, and Mark Greenwald2
1Psychiatry and Radiology, Yale University School of Medicine, New Haven, CT, United States, 2Psychiatry and Behavioral Neurosciences, Wayne State University School of Medicine, Detroit, MI, United States
Synopsis
Separately, acute stress and cigarette cues are associated with cigarette smoking relapse, and each has been shown to increase nicotine seeking/self-administration. However, their potentially additive effects are understudied in humans. Using functional neuroimaging and a placebo-controlled double-blind design, we found acute stress suppressed cue-evoked activation in the medial orbitofrontal, parietal, and prefrontal cortices. Further, the effects of stress on nicotine withdrawal severity were inversely related to medial orbitofrontal and nucleus accumbens activation. Our findings illustrate acute stress exerts cooperative modulation of neural signals and subjective withdrawal severity, known to be important for long-term abstinence.
Background
Tobacco use is the leading cause of preventable death in the United States4. The majority of cigarette smokers relapse within the first year of treatment5-9. Acute stress and smoking cues are often precipitating factors of smoking relapse10-15. Indeed, experimental studies reliably demonstrate both acute stress16-18 and smoking cues17,19,20, separately, increase nicotine seeking/self-administration, a direct measure of nicotine motivation. However, few human studies have examined their potentially additive effects21,22. The goal of this study was to isolate the effects of acute stress on cigarette cue-evoked neural activation during a simple attention-control task.Methods
Non-treatment-seeking cigarette smokers (expired carbon monoxide ≥5ppm, ≥10 cigarettes/day, and Fagerstrom23 score ≥4) without psychiatric comorbidities or cardiovascular/magnetic resonance imaging [MRI] contraindications were eligible. Subjects (N=21) completed two placebo-controlled, double-blind, random cross-over oral-dosing sessions: acute stress (yohimbine 54mg + hydrocortisone 10mg; YOH+HYD) and placebo (0mg, 0mg). Each subject served as his/her own control. Experimental sessions occurred on non-consecutive weekdays between 11am-4pm (Figure 1). Subjects only smoked at designated times during each session (ad libitum before/after sessions). From 1-2pm, participants completed an MRI scan with T1-weighted (MPRAGE) and gradient echo planar imaging (TE=36ms, TR=2.83s, matrix=80x80, 40 interleaved slices, voxel=2.9mm isotropic). Two tasks were administered: N-back and cerebrovascular reactivity (Figure 2). Raw fMRI data were slice-time corrected, motion-corrected, high-pass filtered (128Hz), coregistered to MNI space, smoothed (6mm Gaussian kernel), and resliced (1.5mm isotropic) in SPM8. Within each subject and session, first-level contrast maps (smoking>neutral images for 0- and 1-back, separately) were submitted to group-level, random-effects analyses (cluster-level corrected; AFNI 3dClustSim; p<.05). Mean cluster extents were extracted from first-level contrast maps (smoking>neutral images; 0- and 1-back) for regions of interest (ROIs): medial orbitofrontal cortex (mOFC), insula, and nucleus accumbens (NAcc). Cerebrovascular reactivity (CVR) maps (breath-hold>paced breathing) were contrasted by session (stress>placebo) using a liberal threshold (voxel-level; p<.05) and subtracted from N-back maps to remove potential vascular (non-neural) confounds. Finally, the choice progressive ratio task consisted of 11 independent choice trials during which subjects could earn (via computer ‘mouse’ clicks) either: one cigarette puff or money ($0.25). After the task, subjects smoked the exact number of puffs earned (preferred cigarette brand; live video-verified).Results
Relative to placebo, YOH+HYD significantly increased heart rate, blood pressure, and saliva cortisol (Figure 3). N-back response accuracy was generally high (85%-100%) and did not differ by session (p=.22) or image type (p=.40). After scanning, self-reported appetitive craving, relief-motivated craving, and withdrawal severity was moderate, and did not differ between sessions (p’s=.54, .71, and .84, respectively). Relative to placebo, acute stress significantly increased nicotine seeking/self-administration (p<.05; partial η2=0.24; moderate-to-large effect), controlling for nicotine dependence level (Fagerstrom score). Acute stress suppressed activation: especially in the mOFC, parietal, and prefrontal cortices (Figure 4). Acute stress effects were isolated by calculating difference scores (stress minus placebo) for ROI cluster extents and subjective effects. Exploratory Pearson correlations indicated mOFC and NAcc activation were both inversely correlated with withdrawal severity (Pearson=-.58 and -.50; Figure 5). Controlling for nicotine dependence level and past-week smoking frequency, linear regressions confirmed activation relationships with withdrawal and relief-motivated craving, but not appetitive craving (R2=.49 and .47, respectively). No significant relationships were observed for craving.Discussion
Our findings support the predictive validity of this pharmacological stress-induction approach: YOH+HYD induced a physiological stress response and increased nicotine seeking/self-administration, relative to placebo. Acute stress suppressed activation throughout the cortex, but did not modulate overall nicotine withdrawal severity or cigarette craving levels. However, bivariate correlations, and follow-up linear regressions, indicated the effect of stress on mOFC and NAcc activation was inversely related to withdrawal severity. These findings illustrate the heterogeneous effect of acute stress on important subjective constructs (craving and withdrawal), but the cooperative effects on neural signals in brains regions associated with cue processing (mOFC) and appetitive craving (NAcc)24,25. We speculate that subjects who experienced greater withdrawal severity may have actively suppressed cigarette cue salience/appraisal (mOFC activation) in order to minimize appetitive craving (NAcc activation) which could not be sated during MRI scanning. Importantly, these relationships remained significant after controlling for potential confounds (nicotine dependence level and recent smoking frequency). It must be noted that YOH+HYD is vasoconstrictive (Figure 3), yet CVR difference maps (Figure 4) indicate greater activation during stress (>placebo; especially in the cortex). Thus, we believe stress-induced activation suppression was not an artifact of vasoconstrictive effects. This study examined two factors (stress, cues) known to precipitate smoking relapse, and found the effects of acute stress on craving/withdrawal were specific to the individual, but exhibited strong relationships with neural signals.Acknowledgements
The authors thank Caroline Zajac-Benitez, Muzamil Arshad, Chaitali Anand, Jonathan Lynn, Andrew Neff, Lisa Sulkowski, and Paul Burghardt for their assistance.References
1 Cox, L. S., Tiffany, S. T. & Christen, A. G. Evaluation of the brief questionnaire of smoking urges (QSU-brief) in laboratory and clinical settings. Nicotine & Tobacco Research 3, 7-16 (2001). 2 Wilson, S. J., Sayette, M. A., Fiez, J. A. & Brough, E. Carry-over effects of smoking cue exposure on working memory performance. Nicotine & tobacco research 9, 613-619 (2007). 3 Hughes, J. R. & Hatsukami, D. Signs and symptoms of tobacco withdrawal. Archives of general psychiatry 43, 289-294 (1986). 4 Health, U. D. o. & Services, H. The health consequences of smoking—50 years of progress: a report of the Surgeon General. Atlanta, GA: US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health 17 (2014). 5 Eisenberg, M. J. et al. Pharmacotherapies for smoking cessation: a meta-analysis of randomized controlled trials. Canadian Medical Association Journal 179, 135-144 (2008). 6 Mills, E. J. et al. Comparisons of high-dose and combination nicotine replacement therapy, varenicline, and bupropion for smoking cessation: a systematic review and multiple treatment meta-analysis. Annals of medicine 44, 588-597, doi:10.3109/07853890.2012.705016 (2012). 7 Ucar, E. Y. et al. Effectiveness of pharmacologic therapies on smoking cessation success: three years results of a smoking cessation clinic. interventions 4, 5 (2014). 8 Nides, M. et al. Varenicline versus bupropion SR or placebo for smoking cessation: a pooled analysis. American journal of health behavior 32, 664-675 (2008). 9 Silagy, C., Lancaster, T., Stead, L., Mant, D. & Fowler, G. Nicotine replacement therapy for smoking cessation (Review). (2005). 10 Heishman, S. J. Behavioral and cognitive effects of smoking: relationship to nicotine addiction. Nicotine & Tobacco Research 1, S143-S147 (1999). 11 Matheny, K. B. & Weatherman, K. E. Predictors of smoking cessation and maintenance. Journal of clinical psychology 54, 223-235 (1998). 12 al'Absi, M. Hypothalamic-pituitary-adrenocortical responses to psychological stress and risk for smoking relapse. International journal of psychophysiology : official journal of the International Organization of Psychophysiology 59, 218-227, doi:10.1016/j.ijpsycho.2005.10.010 (2006). 13 Hughes, J. R. Smokers' beliefs about the inability to stop smoking. Addictive behaviors 34, 1005-1009 (2009). 14 Shiffman, S. et al. Immediate antecedents of cigarette smoking: an analysis from ecological momentary assessment. Journal of abnormal psychology 111, 531 (2002). 15 Shiffman, S. Relapse following smoking cessation: a situational analysis. Journal of consulting and clinical psychology 50, 71 (1982). 16 Mantsch, J. R., Baker, D. A., Funk, D., Lê, A. D. & Shaham, Y. Stress-induced reinstatement of drug seeking: 20 years of progress. Neuropsychopharmacology : official publication of the American College of Neuropsychopharmacology 41, 335-356 (2016). 17 Feltenstein, M. W., Ghee, S. M. & See, R. E. Nicotine self-administration and reinstatement of nicotine-seeking in male and female rats. Drug and alcohol dependence 121, 240-246 (2012). 18 Buczek, Y., Le, A., Wang, A., Stewart, J. & Shaham, Y. Stress reinstates nicotine seeking but not sucrose solution seeking in rats. Psychopharmacology 144, 183-188 (1999). 19 Liu, X., Caggiula, A. R., Palmatier, M. I., Donny, E. C. & Sved, A. F. Cue-induced reinstatement of nicotine-seeking behavior in rats: effect of bupropion, persistence over repeated tests, and its dependence on training dose. Psychopharmacology 196, 365-375 (2008). 20 Liu, X. et al. Reinstatement of nicotine-seeking behavior by drug-associated stimuli after extinction in rats. Psychopharmacology 184, 417-425 (2006). 21 Dagher, A., Tannenbaum, B., Hayashi, T., Pruessner, J. C. & McBride, D. An acute psychosocial stress enhances the neural response to smoking cues. Brain research 1293, 40-48, doi:10.1016/j.brainres.2009.07.048 (2009). 22 Potenza, M. N. et al. Neural correlates of stress-induced and cue-induced drug craving: influences of sex and cocaine dependence. The American journal of psychiatry 169, 406-414, doi:10.1176/appi.ajp.2011.11020289 (2012). 23 Heatherton, T. F., Kozlowski, L. T., Frecker, R. C. & FAGERSTROM, K. O. The Fagerström test for nicotine dependence: a revision of the Fagerstrom Tolerance Questionnaire. British journal of addiction 86, 1119-1127 (1991). 24 Chase, H. W., Eickhoff, S. B., Laird, A. R. & Hogarth, L. The neural basis of drug stimulus processing and craving: an activation likelihood estimation meta-analysis. Biological psychiatry 70, 785-793 (2011). 25 Wilson, S. J., Sayette, M. A. & Fiez, J. A. Prefrontal responses to drug cues: a neurocognitive analysis. Nature neuroscience 7, 211-214 (2004).Figures
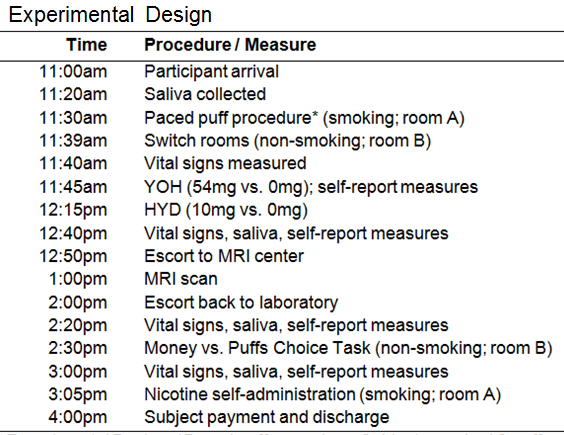
Experimental Design. *Paced puff procedure: Subjects smoked 6 puffs over 5 minutes to control for recent nicotine exposure (preferred cigarette brand; live video verified).
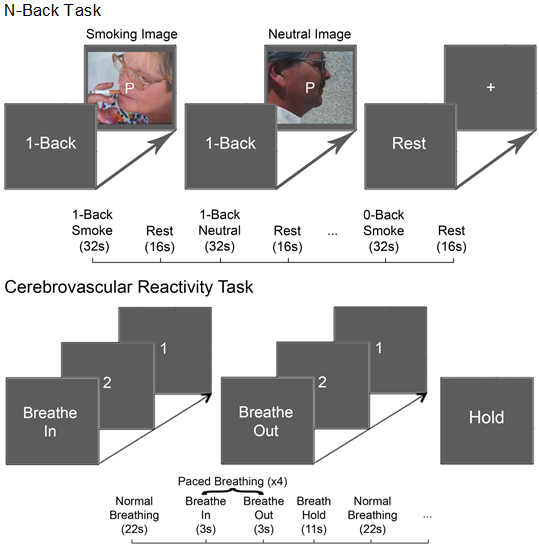
fMRI Tasks: (Top) The N-back task consisted of an
instructional prompt (2s) prior to 30s blocks of letter 0- and 1-back
(3s/image) yoked with cigarette smoking or neutral, non-smoking images (matched
for visual characteristics). Two blocks per condition were presented in
pseudo-random order and separated by 16s of blank screen to minimize carry-over
effects2. (Bottom) The cerebrovascular reactivity
task consisted of 5 repetitions of each:
normal/uncontrolled breathing (22.64s), 4 repetitions of paced breathing
(~3s/in, ~3s/out; 22.64s total), and breath hold (11.32s).
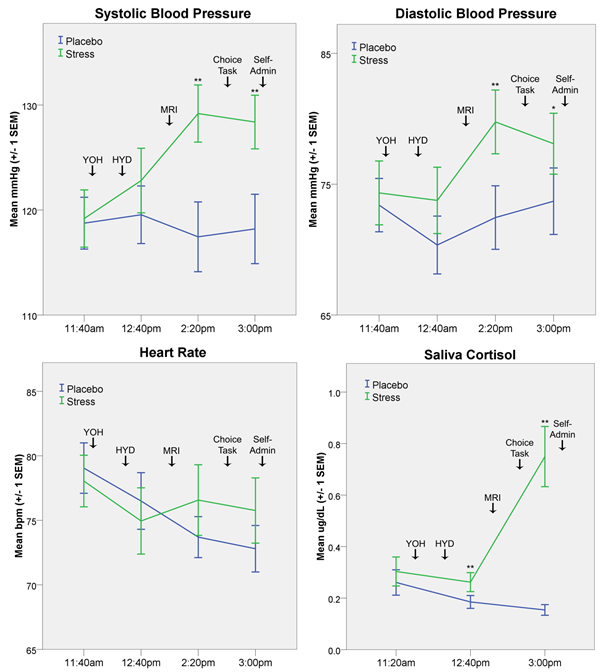
Physiological Effects:
Repeated measures analyses of variance indicated that YOH+HYD
significantly increased systolic and diastolic blood pressure, heart rate, and
saliva cortisol levels throughout the stress session, relative to placebo
levels (Dose X Time interactions; ps
< .05). Significant between-session pairwise differences indicated with
asterisks: *p<.05 and **p<.01.
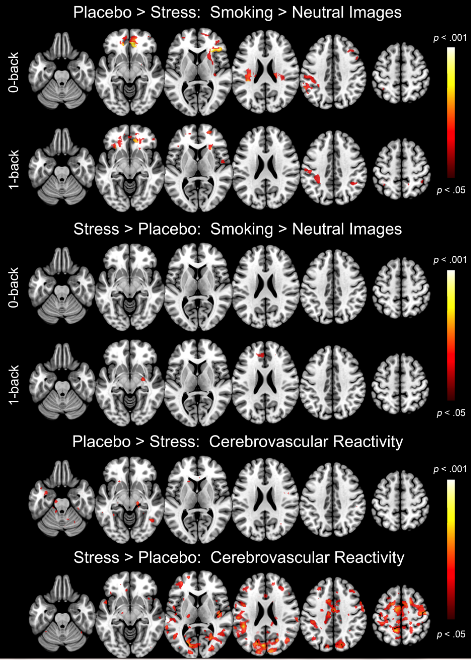
fMRI Activation Maps:
(Upper) Cluster-level (AFNI
3dClustSim; p<.05) and
cerebrovascular reactivity-corrected activation maps contrasted by session are
depicted on contiguous axial slices separately for each N-back level. (Lower) Cerebrovascular reactivity
(breath-hold > paced breathing) activation maps contrasted by session (voxel-level;
p<.05) are depicted on contiguous
axial slices. Color bars indicate significance.
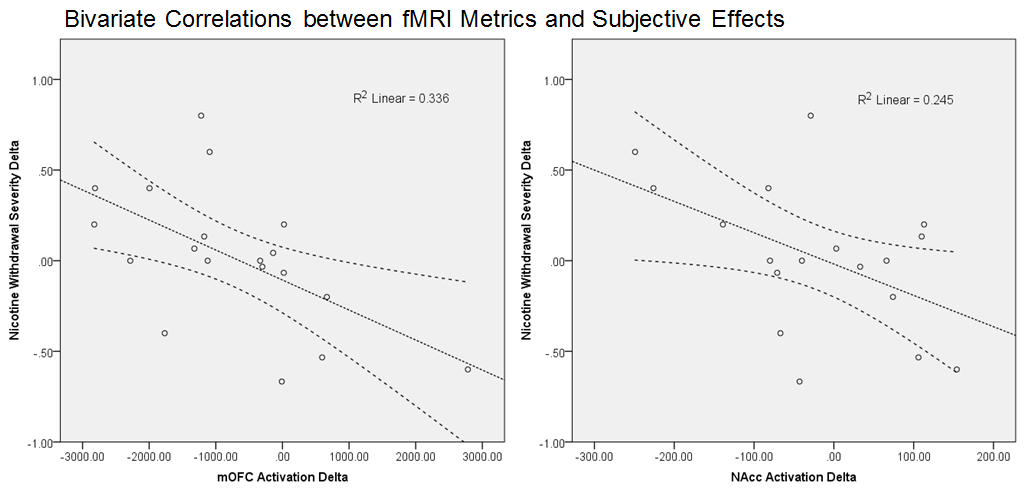
Bivariate Correlations: Mean cluster extents were extracted from ROIs
(insula, mOFC, and NAcc) from first-level contrast maps (smoking > neutral
images; 0- and 1-back combined). Self-reported appetitive cigarette craving
(Questionnaire for Smoking Urges; QSU1), relief-motivated
craving (QSU), and nicotine withdrawal symptom severity (Minnesota Nicotine
Withdrawal Scale; MNWS3) were collected
following the MRI scan and before nicotine seeking (Choice Task). Difference
scores (stress minus placebo; ‘deltas’)
were calculated and evaluated with bivariate correlations. Linear regressions,
controlling for potential confounds (nicotine dependence and past-week smoking
frequency), confirmed two significant relationships (above).