2261
Tomoelastography of pancreatic tumors: Preliminary results1Radiology, Charité - Universitätsmedizin Berlin, Berlin, Germany, 2Experimental Surgery, Charité - Universitätsmedizin Berlin, Berlin, Germany, 3Medical Informatics, Charité - Universitätsmedizin Berlin, Berlin, Germany
Synopsis
High-resolution stiffness maps of the pancreas were generated using multifrequency magnetic resonance elastography (MRE) and tomoelastography data processing in healthy controls (Ctr) and patients with pancreatic carcinoma (Pa-Ca). Pa-Ca have higher stiffness than control tissue and non-tumorous pancreatic parenchyma in patients without overlap to normal values. Subregional analysis for pancreatic head, corpus and tail revealed no difference between these anatomical regions. Tomoelastogaphy is sensitive to pathological changes in viscoelastic properties of Pa-Ca and offers a quantitative measure of stiffness of pancreatic tissue.
Purpose:
To investigate pancreatic stiffness noninvasively in patients with pancreatic carcinoma (Pa-Ca) using multi-frequency magnetic resonance elastography (MRE) and tomoelastography data processing.Background:
Pa-Ca are highly-aggressive tumors with a high mortality. Surgery remains the only curative treatment option. Tumor size and location determine respectability and treatment success. Current imaging methods are limited in providing sufficient information for Pa-Ca treatment.Methods:
Six patients (67±11 years, 2 females) with confirmed Pa-Ca and eight healthy controls (30±7 years, 3 females) were prospectively enrolled in the study. Multifrequency MRE (1) and T2w-imaging were performed in each subject. All experiments were conducted on a 1.5-T MRI scanner equipped with a 12-channel phased array surface coil. Mechanical vibrations were induced by three pressurized air driven actuators. Vibration frequencies were 30, 40, 50 and 60 Hz. Imaging parameters were the same as described in (2). All imaging protocols were executed in an axial slice orientation covering the entire pancreas with free breathing. MRE data post-processing was based on the tomoelastography pipeline detailed in (3), yielding wave speed maps (elastograms) in m/s. Selection of the regions of interest (ROI) and parameter averaging were done with Image J v1.50i. ROIs were placed inside the tumor (Pa-Ca) and in non-tumorous pancreatic parenchyma (Pa-NT). In Ctr MRE parameters of the pancreatic head, corpus and tail were evaluated separately.Results:
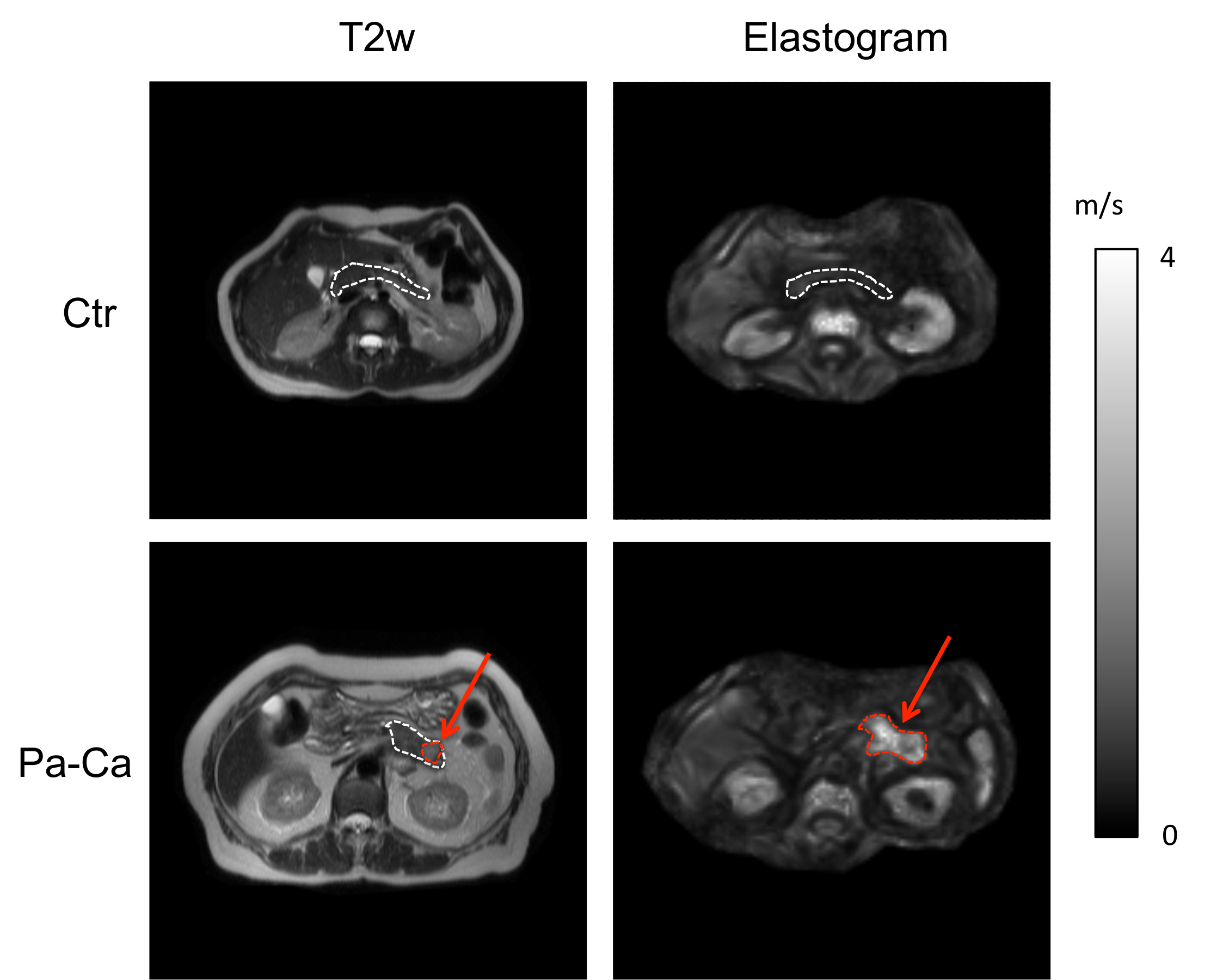
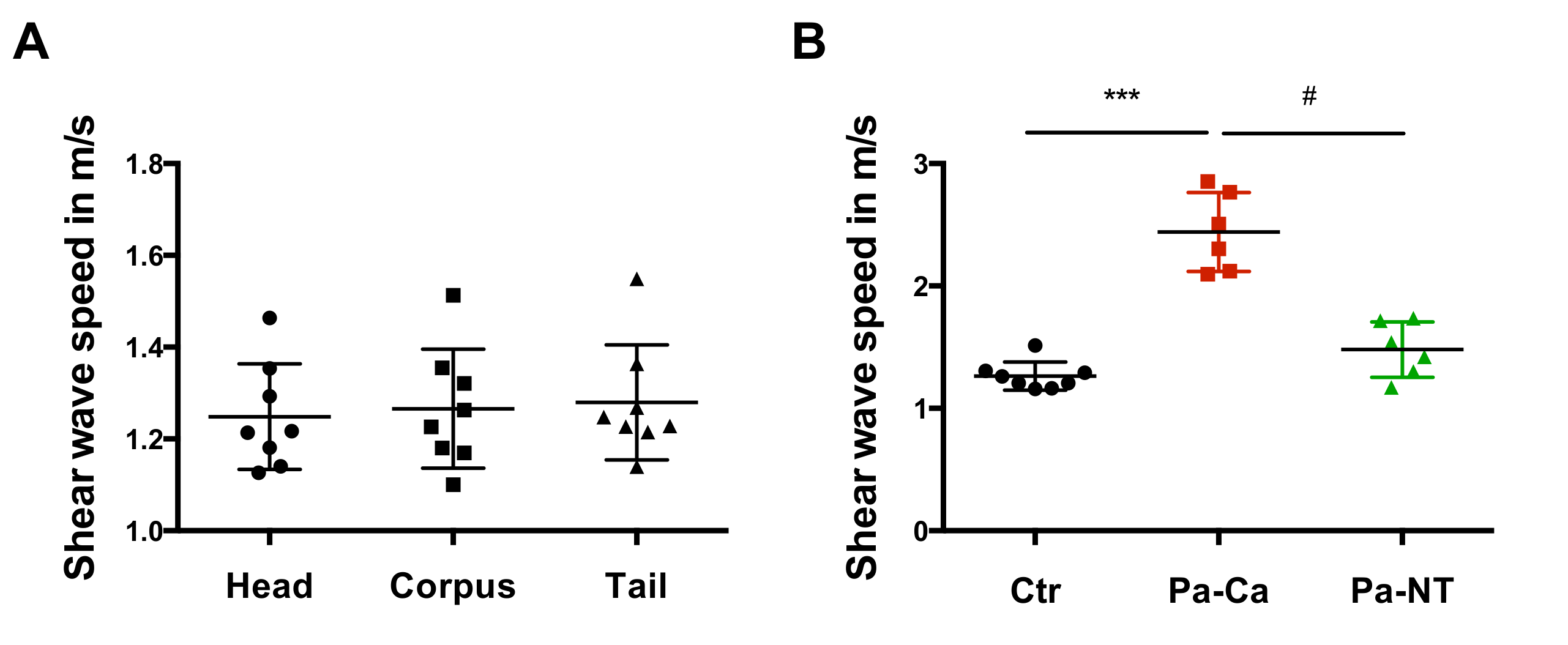
Tomoelastography revealed to the naked eye stiff tumor regions in all patients. T2w imaging showed a distinct tumor area only in one patient. Fig 1 shows the MRE magnitude image (T2w) and wave speed map (elastogram) of one healthy volunteer and one patient with Pa-Ca in MRE- and T2w-images. In contrast to T2w-images (diameter, 20 × 16 mm mm), MRE (diameter, 52 × 31 mm) predicts a bigger tumor size. In the elastogram, the Pa-Ca has an apparently higher shear wave speed than the pancreas of the healthy volunteer. As no significant difference between the pancreas head (1.25 ± 0.12 m/s), corpus (1.27 ± 0.13 m/s) and tail (1.28 ± 0.13 m/s) were obtained in Ctr, data from all pancreatic subregions were pooled for further group analysis. Group mean values of wave speed obtained from MRE are significantly higher (P <0.001) in patients with Pa-Ca (2.44 ± 0.32 m/s) than in healthy volunteers (mean of the entire pancreas, 1.26 ± 0.11 m/s) and inner-patient, non-tumorous parenchyma (1.48 ± 0.23 m/s; P = 0.03), respectively. Pa-NT did not differ from Ctr (see Fig. 2).Discussion:
In this preliminary study, we applied a multi-parametric imaging protocol to patients with pancreatic carcinoma and healthy controls. MRE values for healthy volunteers are consistent with previous reports based on similar imaging parameters using multi- (2) and single-frequency at 60 Hz (4). In healthy volunteers we did not observed a difference in subregional analysis, which agrees with a currently published MRE study (4). High-resolution stiffness maps allow a differentiation from Pa-Ca and Pa-NT. Pa-Ca are associated with a strong increase in stiffness, represented by higher shear wave speed values compared to healthy volunteers. Remarkably, there was no overlap of values between Pa-Ca stiffness and normal tissue in our study. Pa-Ca in our study appeared bigger than in conventional T2-weighted MR-images. More patients will be recruited in this ongoing study and imaging parameters will be correlated with clinical and histopathological findings.Conclusion:
Tomoelastography of the pancreas promises to be a valuable diagnostic tool for characterization of pancreatic tumors and detection of tumor boundaries. No subregional differences of pancreatic stiffness were observed in this study. Pancreatic carcinomas are stiffer than non-tumorous parenchyma or normal tissue without overlap of values.Acknowledgements
No acknowledgement found.References
1. Muthupillai R, Ehman RL. Magnetic resonance elastography. Nat Med 1996;2(5):601-603.
2. Dittmann F, Tzschatzsch H, Hirsch S, Barnhill E, Braun J, Sack I, Guo J. Tomoelastography of the abdomen: Tissue mechanical properties of the liver, spleen, kidney, and pancreas from single MR elastography scans at different hydration states. Magn Reson Med 2017;78(3):976-983.
3. Tzschatzsch H, Guo J, Dittmann F, Hirsch S, Barnhill E, Johrens K, Braun J, Sack I. Tomoelastography by multifrequency wave number recovery from time-harmonic propagating shear waves. Med Image Anal 2016;30:1-10.
4. Kolipaka A, Schroeder S, Mo X, Shah Z, Hart PA, Conwell DL. Magnetic resonance elastography of the pancreas: Measurement reproducibility and relationship with age. Magn Reson Imaging 2017;42:1-7.
Figures