2258
Morphometric Adaptions of Rectus Femoris to Muscle Strain Revealed Through ‘Dynamic Magnetic Resonance Elastography’ (DMRE)1MRC Centre for Inflammation Research, University of Edinburgh, Edinburgh, United Kingdom, 2Edinburgh Imaging Facility, University of Edinburgh, Edinburgh, United Kingdom, 3Department of Clinical Surgery, University of Edinburgh, Edinburgh, United Kingdom, 4Department of Bioengineering, University of Strathclyde, Glasgow, United Kingdom, 5The Mentholatum Company Ltd., East Kilbride, Glasgow, United Kingdom, 6Department of Trauma & Orthopeadic Surgery, University of Manchester, Manchester, United Kingdom
Synopsis
Magnetic Resonance Elastography (MRE) allows for the quantification of tissue stiffness. When MRE is applied in muscle it allows for the measurement of muscle strain, with strain having an impact on structure morphology. This research investigated whether the bi-articular design of the Rectus Femoris gives an anatomical advantage in adapting to muscle strain and avoiding injury, as this is a vital muscle for movement. It was found that the mono-articular Quadriceps muscles showed significant muscle strain from loading, whereas the Rectus Femoris showed significant changes in cylindrical shape, and as expected, adapted to increased loading.
Introduction
Magnetic Resonance Elastography (MRE) allows for the quantification of tissue stiffness1,2 and is finding increasing clinical application3. Furthermore, MRE allows muscle strain to be computed4,5 and can provide insight regarding physiological changes under muscle loading6. In addition, muscle shape changes may also be measured using conventional MRI7. Due to muscle being a tissue that can be readily manipulated, muscle loading can offer significant insight into muscle physiology8, for instance the change in the shape of structures in strain9. Measuring muscle morphology and mechanical properties at different levels of strain allows for a dynamic appreciation of muscle physiology, leading to a newly developed technique called ‘Dynamic Magnetic Resonance Elastography’ (DMRE). The aim of present study was to investigate whether the shape of the Rectus Femoris changes in response to increased loading and muscle strain through DMRE. The hypothesis of this research is that the bi-articular design of the Rectus Femoris will allow it to change shape in response to loading and potentially allow it to withstand greater levels of strain without injury.Methods
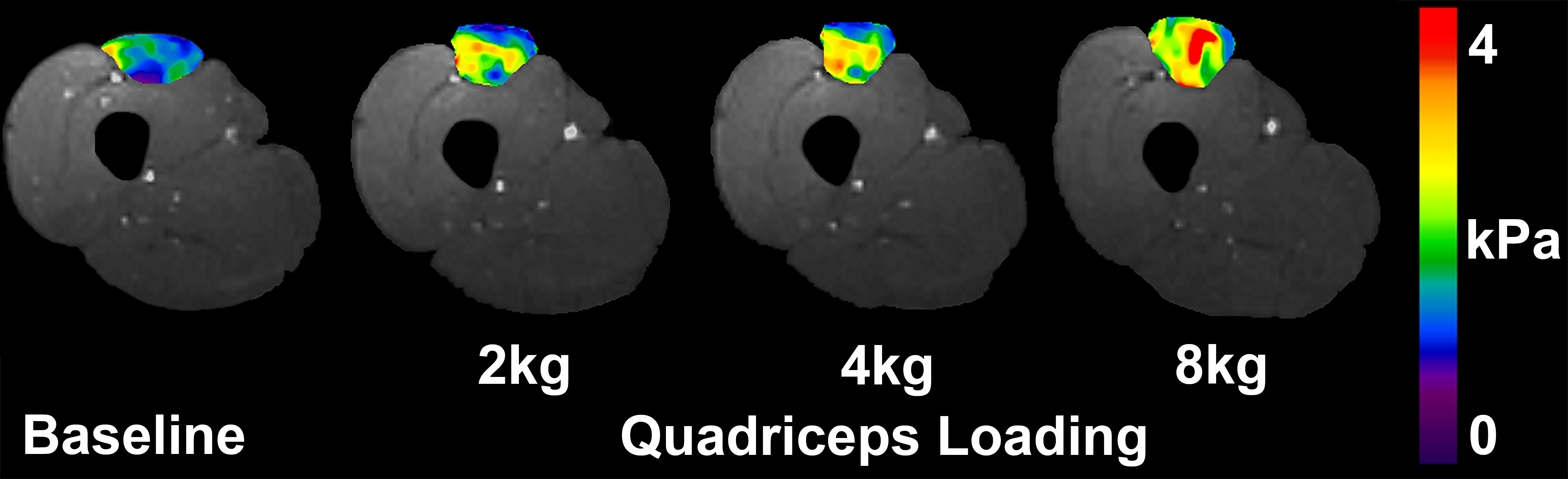
An MRI muscle loading paradigm was designed where the knees of participants (33.00[±9.06] years, n=4) were initially flexed at 50°, and subsequently partially extended to 25°. A custom designed muscle loading apparatus allowed the Quadriceps to be loaded at increasing intervals (2kg, 4kg and 8kg) during concentric knee extensions. The apparatus limited lower leg extension to 25°, and so ensured participants extended consistently for each trial and enabled sustained loading during image acquisition (80sec). MRE actuation was performed using a Resoundant system (Resoundant, Mayo Clinic, Rochester, MN, USA) which was attached through a non-inflated tourniquet cuff around the mid-thigh of participants. Multi-frequency MRE10 images were obtained at 25, 37.5 and 50Hz which were post-processed with the ESP inversion algorithm11, to produce maps of muscle stiffness (|G*|). Region of Interest (ROI) analysis of |G*| was performed for the Quadriceps muscle group, as Rectus Femoris, Vastus Intermedius, Vastus Lateralis and Vastus Medialis individually. Measurements were also obtained of muscle cross-sectional area (CSA; cm2) and muscle circularity (4π[Area/Perimeter2]) for a single axial slice. All measures were obtained at baseline and at each loading interval during knee extension. Repeated Measures Multivariate ANOVA (MANOVA) was used to evaluate changes.Results
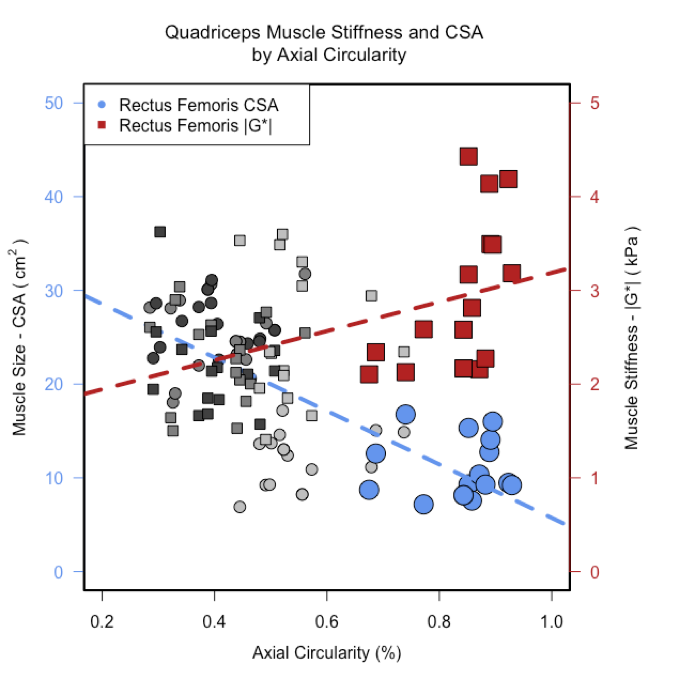
Muscle |G*| in the Quadriceps | significantly increased during loading (+51%; p=.005). Significant |G*| increases during loading in individual muscles were also observed (Figure 1) in Vastus Lateralis (+57%; p=.015) and Vastus Intermedius (+56%; p=.008), however not individually in Vastus Medialis (+45%; p=.293), or the prime mover Rectus Femoris (+50%; p=.195). Morphological changes were observed in Rectus Femoris (Figure 2) with a significant increase in axial muscle circularity during loading (+22%; p=.005), however not for Vastus Medialis (-15%, p=.489), Vastus Lateralis (+1%; p=.999) or Vastus Intermedius (-8%; p=.954). A significant linear correlation was observed for muscle |G*| and circularity in Rectus Femoris (r[14]=.58; p=.019; Figure 3). However, in the Quadriceps muscles as a whole there was a significant positive correlation between muscle circularity and |G*| (r[62]=.44; p<.000), and a negative correlation between muscle circularity and muscle CSA (r[62]=-.70; p<.000; Figure 3). Furthermore, a linear regression was performed for muscle |G*| being a dependent factor from muscle circularity and CSA, showing a significant result for the Quadriceps muscles (R2=.20, F(3,60)=4.88, p=.004).Discussion
Rectus Femoris is the primary muscle for concentric knee extensions, thus, it was expected that this muscle in particular would be prone to muscle strain. During loading, there was not a significant increase in muscle |G*|, but instead the muscle became more circular and decreased in CSA in an axial slice. These results provide evidence that the bi-articular anatomy and limited connection to the femur, allows the Rectus Femoris to adapt morphometrically to increased muscle strain in order to avoid muscle damage.Conclusion
The use of DMRE has offered a unique insight into muscle physiology in relation to morphology. Use of DMRE in profiling muscle strain has future clinical applications in identifying physiological reasoning for patients being prone to injury, or slow to recover. Future clinical research should incorporate dynamic muscle measurements in order to achieve a full appreciation of muscle health.Acknowledgements
No acknowledgement found.References
1. Muthupillai R, Lomas DJ, Rossman PJ, Greenleaf JF, Manduca A, Ehman RL. Magnetic resonance elastography by direct visualization of propagating acoustic strain waves. Science. 1995 Sep 29:1854-7.
2. Manduca A, Oliphant TE, Dresner MA, Mahowald JL, Kruse SA, Amromin E, Felmlee JP, Greenleaf JF, Ehman RL. Magnetic resonance elastography: non-invasive mapping of tissue elasticity. Medical image analysis. 2001 Dec 31;5(4):237-54.
3. Mariappan YK, Glaser KJ, Ehman RL. Magnetic resonance elastography: a review. Clinical anatomy. 2010 Jul 1;23(5):497-511.
4. Bensamoun SF, Ringleb SI, Littrell L, Chen Q, Brennan M, Ehman RL, An KN. Determination of thigh muscle stiffness using magnetic resonance elastography. Journal of Magnetic Resonance Imaging. 2006 Feb 1;23(2):242-7.
5. Ringleb SI, Bensamoun SF, Chen Q, Manduca A, An KN, Ehman RL. Applications of magnetic resonance elastography to healthy and pathologic skeletal muscle. Journal of Magnetic Resonance Imaging. 2007 Feb 1;25(2):301-9.
6. Perrins M, Barnhill E, Braun J, Sack I, Hunter A, Brown C, van Beek EJR, Roberts N. Super-Resolution Magnetic Resonance Elastography (SR-MRE) of Exercise Induced Muscle Damage (EIMD). Proc. Intl. Soc. Magn. Reson. Med., (5981), 2016
7. Perrins M, Hiscox L, Gray C, Semple S, Barclay L, Kirkbride R, Salisbury L, Brown C, Walsh T, van Beek EJR, Roberts N, Griffith D. Muscle Change Associated with Time in Intensive Care Unit (ICU). Proc. Intl. Soc. Magn. Reson. Med., (5069), 2017
8. Dresner MA, Rose GH, Rossman PJ, Muthupillai R, Manduca A, Ehman RL. Magnetic resonance elastography of skeletal muscle. Journal of Magnetic Resonance Imaging. 2001 Feb 1;13(2):269-76.
9. Filon LN. On the elastic equilibrium of circular cylinders under certain practical systems of load. Philosophical Transactions of the Royal Society of London. Series A, Containing Papers of a Mathematical or Physical Character. 1902 Jan 1;198:147-233.
10. Papazoglou S, Rump J, Braun J, Sack I. Shear wave group velocity inversion in MR elastography of human skeletal muscle. Magnetic resonance in medicine. 2006 Sep 1;56(3):489-97.
11. Barnhill E, Kennedy P, Johnson CL, Mada M, Roberts N. Real‐time 4D phase unwrapping applied to magnetic resonance elastography. Magnetic resonance in medicine. 2015 Jun 1;73(6):2321-31.
Figures