2169
Introducing a fat-image guided registration technique for image-based retrospective motion compensation for free-breathing background suppressed renal pCASL1Center for Image Sciences, University Medical Center Utrecht, Utrecht, Netherlands, 2C.J.Gorter Center for High Field MRI, Leiden University Medical Center, Leiden, Netherlands, 3Radiology, University Medical Center Utrecht, Utrecht, Netherlands
Synopsis
Aiming for rapid and accurate perfusion measurement, background suppressed (BGS) ASL under free breathing is desired. Motion compensation on BGS ASL is challenging due to the lack of anatomical contrast. We investigated the benefit of BGS versus non-BGS ASL, guided by motion compensation based on the ASL-images themselves and additionally acquired fat-images. Registration effect on perfusion weighted signal (PWS) and temporal SNR (tSNR) was evaluated for ASL-image and fat-image based registration, proving increased tSNR and increased PWS robustness, without compromising signal intensity. We conclude that free-breathing BGS renal pCASL with image-based retrospective motion compensation yields better reproducibility than without BGS.
Introduction
Perfusion imaging using subtraction-based arterial spin labeling (ASL) MRI is inherently limited by low SNR and is affected by physiological, image noise and abdominal bulk motion. To overcome these limitations for renal ASL, (1) background suppression (BGS) has been shown to increase sensitivity1 and (2) motion compensation strategies, such as breath-holding, synchronized breathing and image-based registration have been shown to reduce subtraction artifacts2. Aiming for rapid and accurate perfusion measurement, BGS ASL under free breathing (FB) is desired, alleviating patient cooperation for abdominal ASL. However, image-based registration of ASL images might be affected by the lack of anatomical contrast in BGS ASL and therefore the use of surrogate motion signals has been proposed2. Inspired by recent work that employed fat-images for motion compensation of DCE-MRI3,4, we investigated its feasibility for BGS ASL. To this end, we compared BGS versus non-BGS ASL, guided by motion compensation based on the ASL-images themselves and the additional fat-images.Methods
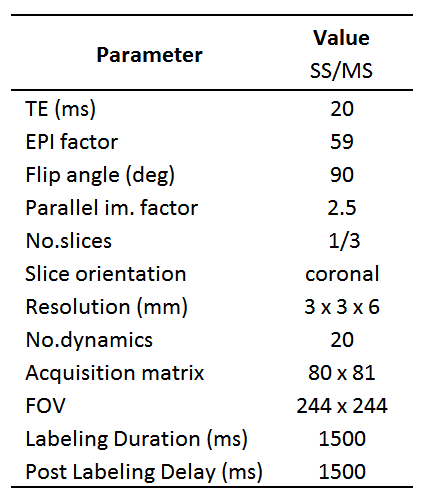
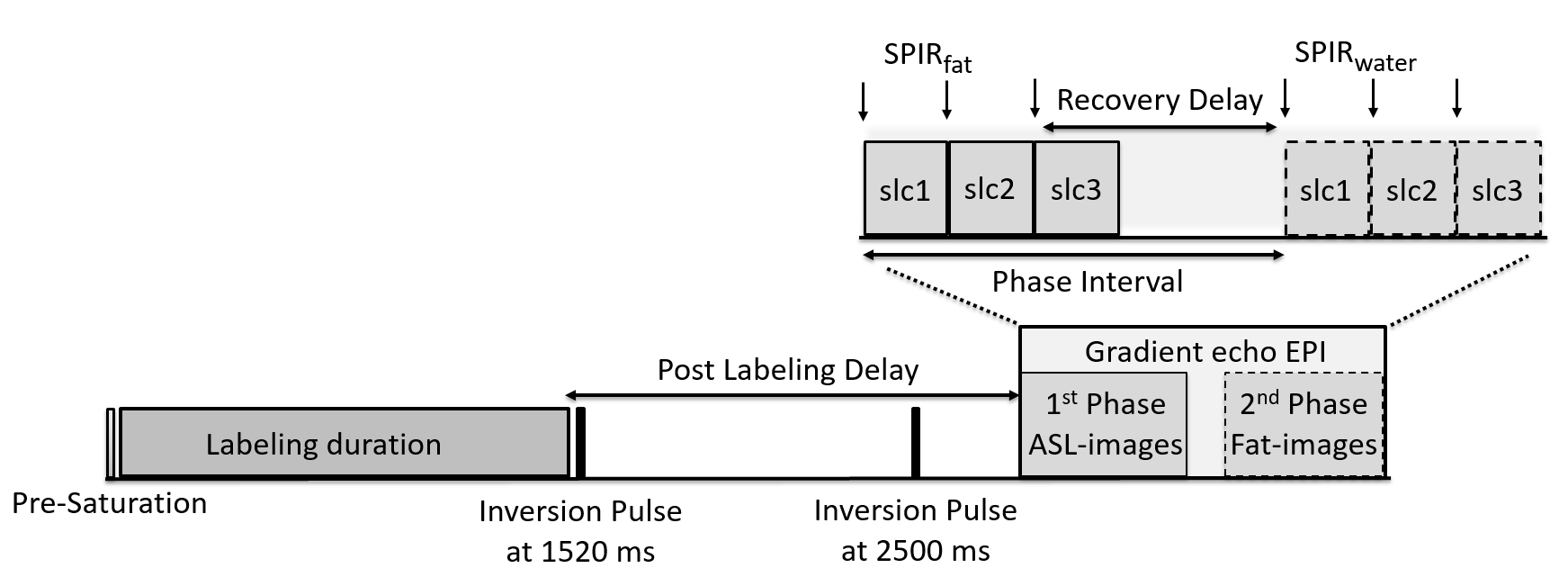
Imaging: Seven volunteers (age 24 - 43, 3 men) were scanned on a 1.5T-MRI (Achieva, Philips, NL) using a 16-element torso coil. Pseudo-continuous ASL (pCASL) was acquired with a gradient echo EPI readout (see Table 1), with background suppression (BGS) and without (non-BGS), in single-slice (SS) and multi-slice (MS; 3slices) acquisitions. BGS using two inversion pulses was optimized to have slightly positive static tissue signal, avoiding sign changes in label images that would corrupt perfusion signal. Within the same sequence, fat-images were acquired as a second phase readout with a phase interval of 200 ms and 324 ms for SS and MS, respectively (Figure 1), allowing the fat signal to recover from saturation of the SPIR fat suppression pulse preceding the regular ASL image acquisition.
Analysis: Prior to registration, fat-images were corrected for the water-fat shift in feet/head direction. Kidneys where manually segmented in the first ASL dynamic. Segmentations served kidney-specific motion compensation and ROI analysis. Motion compensation was performed, for each kidney separately, by rigid registration (3D MS vs 2D SS) of all ASL-images to the first dynamic directly (ASLReg), or via registration of their corresponding fat-images (FatReg). Absence of motion between the ASL and fat-image was assumed. The control image of the non-BGS acquisition served as M0 estimate, and was co-registered via the fat-image to the non-BGS and BGS ASL. After registration, subtraction images were averaged over all dynamics and expressed as relative signal difference to M0, yielding perfusion weighted images (PWIs). Voxel-wise temporal SNR (tSNR) within the ROI of the PWIs was expressed as the ratio of the mean PWI voxel-wise perfusion weighted signal over time and the temporal voxel-wise standard deviation of PWI. tSNR was evaluated as a surrogate for the precision of the perfusion measurement.
Results
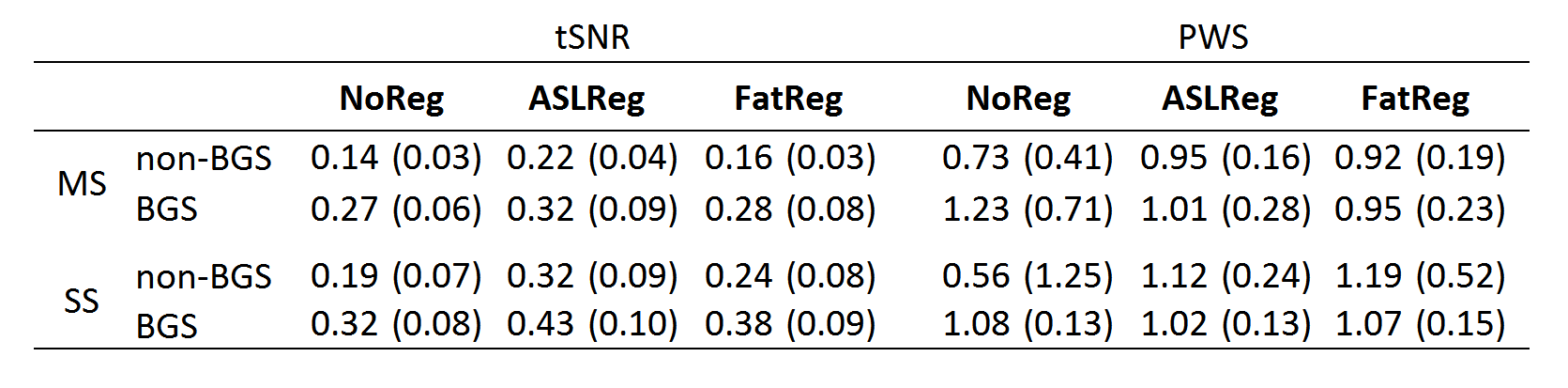
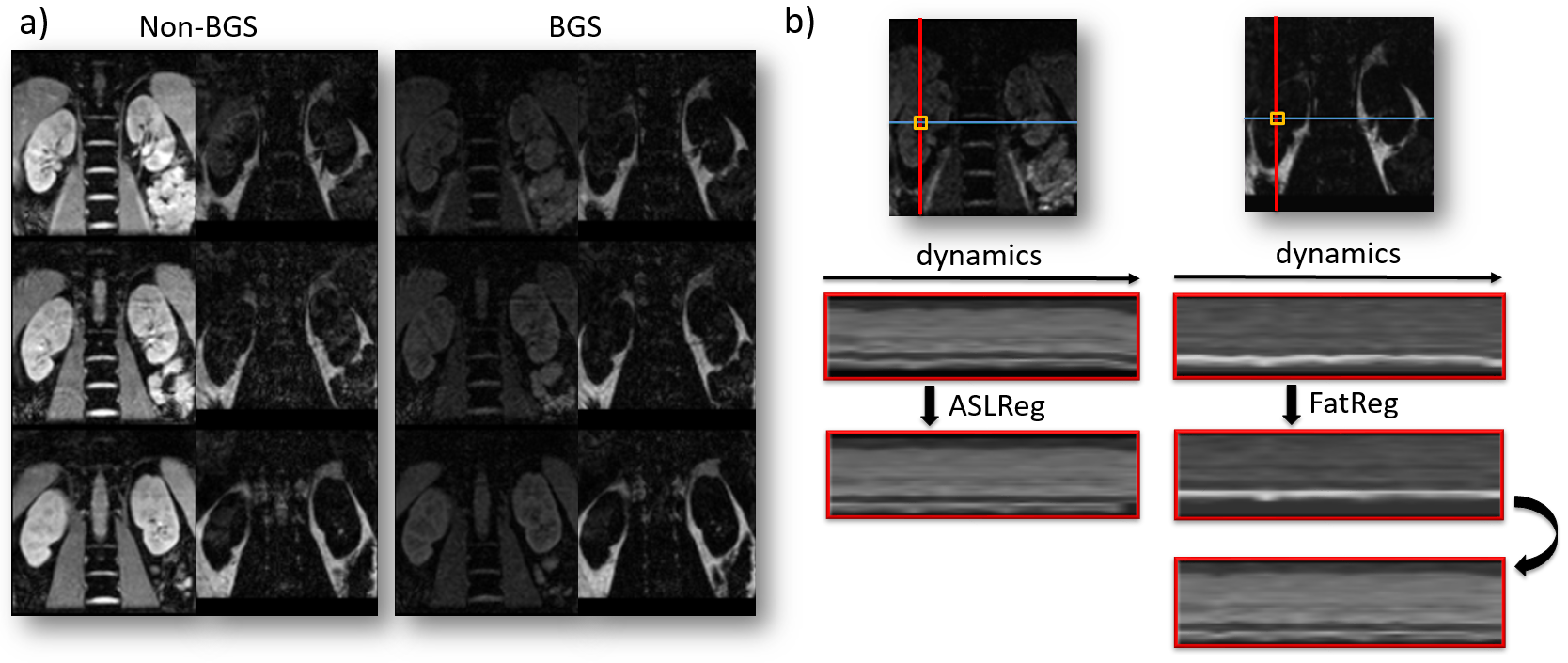
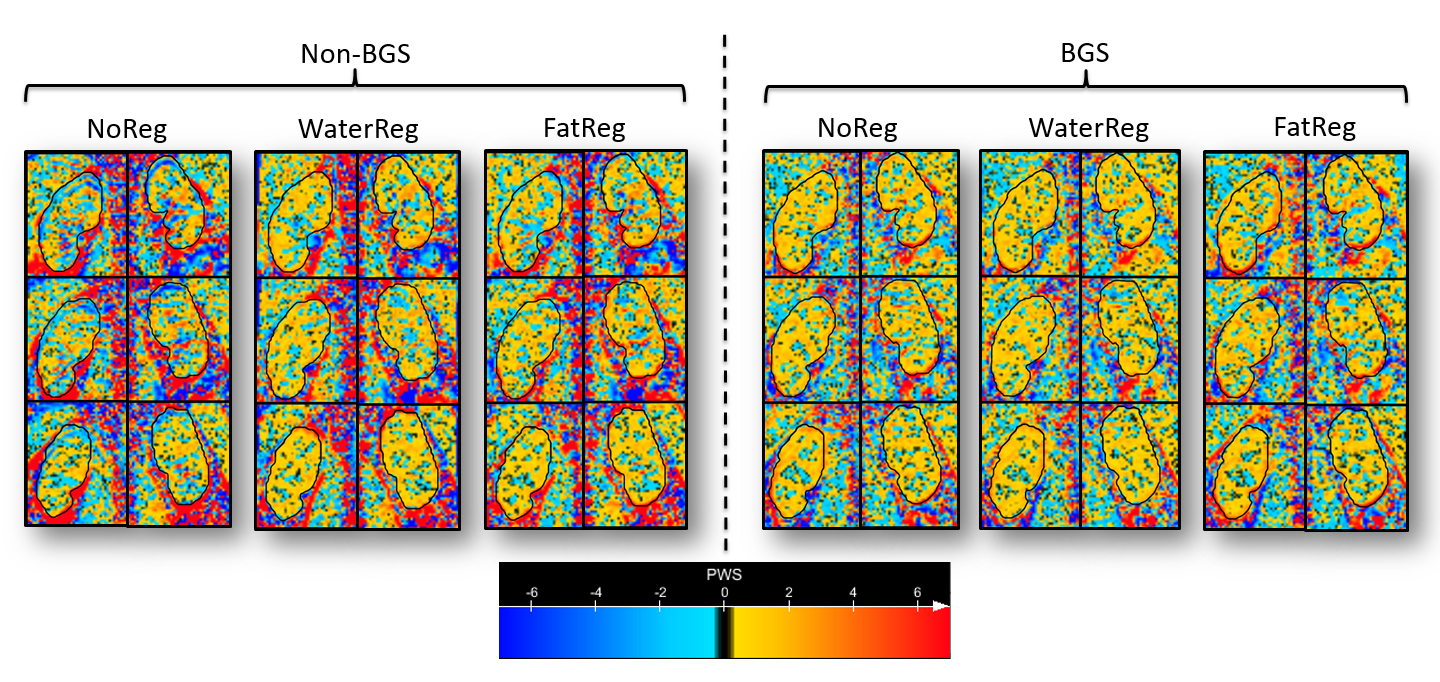
Fat-image guided retrospective motion compensation was accomplished for all seven volunteers, despite varying fat contour quantity (Figure 2). FatReg showed a relative tSNR increase of 17% for MS and SS, respectively, compared with no registration (NoReg), for both MS and SS. The higher tSNR increase for SS series demonstrates that the recovery delay induced kidney position mismatch influences FatReg performance for perfusion weighted signal (PWS). Retrospective image registration significantly improved tSNR using the conventional ASLReg (Wilcoxon, p<0.05) and the proposed FatReg (Wilcoxon, p<0.05) technique compared with NoReg (Table 2). This is consistently reflected in a higher robustness of the PWS, as implied by an improved agreement of ASLReg and FatReg, with and without BGS (Figure 3). Applying BGS resulted in an average tSNR increase of 70% and did not reduce the PWS for either registration technique. Surprisingly, for both non-BGS and BGS, ASLReg yielded better tSNR than FatReg for image registration (Table 2).Discussion and conclusions
This study consistently shows that renal free-breathing BGS pCASL with retrospective motion compensation by image registration improves tSNR, suggesting better reproducibility than non-BGS, without compromising PWS. Overall, tSNR is higher in SS acquired images compared with MS. Surprisingly, ASLReg outperforms FatReg even on the BGS data with limited anatomical contrast. For both registration techniques, tSNR increased and robustness of PWS improved. We anticipate that with more aggressive BGS image-based motion compensation will require guidance by fat-images. FatReg could act similarly for co-registration of the M0 image to BGS data, as was already performed in this study. Future work will focus on minimizing the phase interval to reduce possible motion between ASL and fat-images. Additionally, incorporating complex data subtractions will enable perfusion quantification with more aggressive BGS, maximizing tSNR gain and due to successful FatReg free-breathing motion compensation, alleviating patient cooperation for abdominal ASL.Acknowledgements
This work is part of the research programme Applied and Engineering Sciences with project number 14951 which is (partly) financed by the Netherlands Organisation for Scientific Research (NWO). We thank MeVis Medical Solutions AG (Brehmen, Germany) for providing MeVisLab medical image processing and visualization environment, which was used for image analysis.References
1. Garcia, D. M., Duhamel, G., & Alsop, D. C. (2005). Efficiency of inversion pulses for background suppressed arterial spin labeling. Magnetic Resonance in Medicine, 54(2), 366–372. http://doi.org/10.1002/mrm.20556
2. Robson, P. M., Madhuranthakam, A. J., Dai, W., Pedrosa, I., Rofsky, N. M., & Alsop, D. C. (2009). Strategies for reducing respiratory motion artifacts in renal perfusion imaging with arterial spin labeling. Magnetic Resonance in Medicine, 61(6), 1374–1387. http://doi.org/10.1002/mrm.21960
3. De Boer, A., Leiner, T., & Van den Berg, N. (2017). Automated renal motion correction using fat-images derived from Dixon reconstruction of DCE MRI. In Proceedings of the 25th Annual Meeting of ISMRM 2017:0210
4. Srinivasan, S., Hargreaves, B. A., & Daniel, B. L. (2017). Fat-based registration of breast dynamic contrast enhanced water images. Magnetic Resonance in Medicine, 18, 1307–7. http://doi.org/10.1002/mrm.26851
Figures