2131
Advanced MR imaging characterization of a novel in vivo xenograft model mimicking recurrent glioblastoma1Radiology, Medical College of Wisconsin, Milwaukee, WI, United States, 2Medicine, Medical College of Wisconsin, Milwaukee, WI, United States, 3Neurosurgery, Medical College of Wisconsin, Milwaukee, WI, United States, 4Pediatrics, Medical College of Wisconsin, Milwaukee, WI, United States, 5Neuro-Oncology, Medical College of Wisconsin, Milwaukee, WI, United States, 6Neurology, Medical College of Wisconsin, Milwaukee, WI, United States, 7Chemistry & Biochemistry, University of Wisconsin, Milwaukee, WI, United States, 8Biophysics, Medical College of Wisconsin, Milwaukee, WI, United States
Synopsis
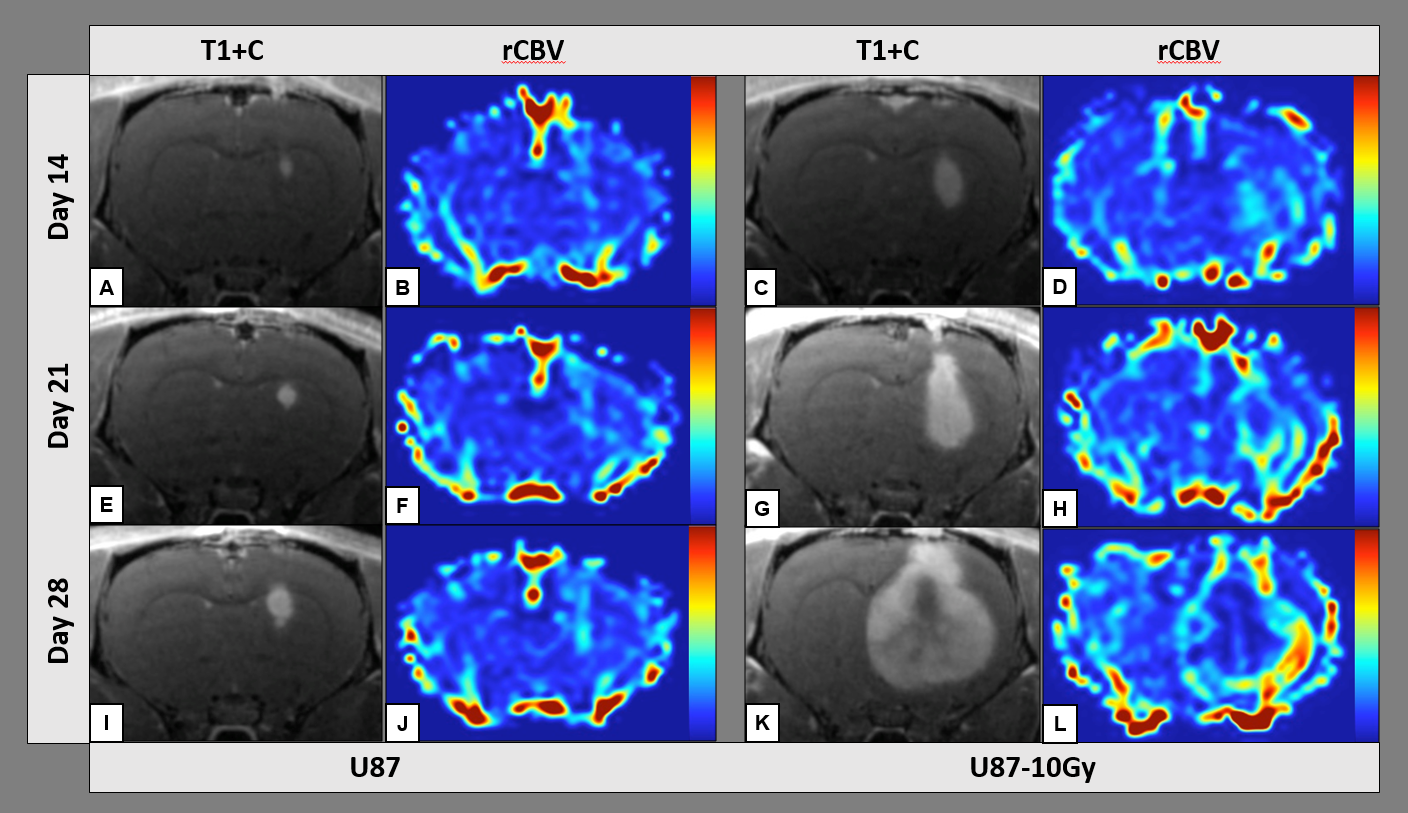
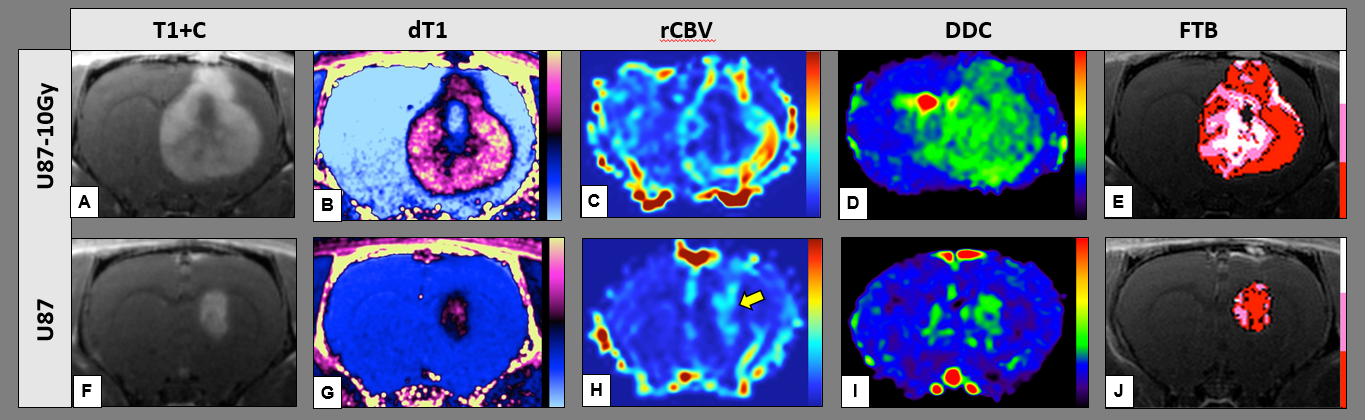
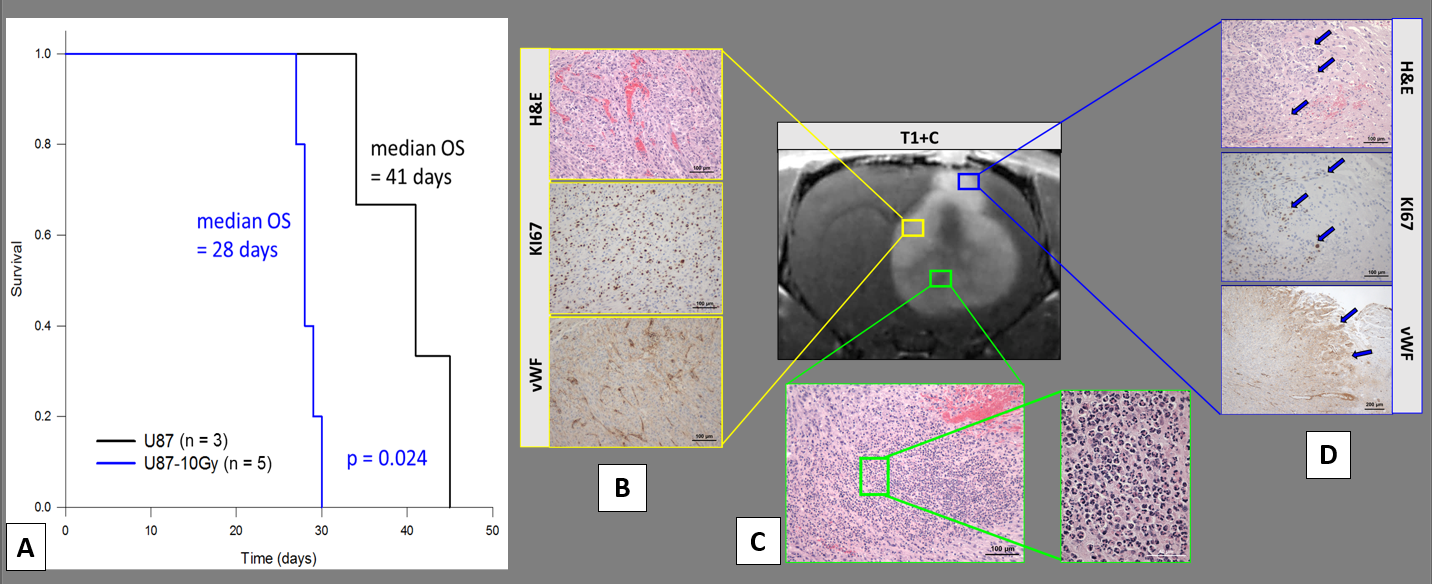
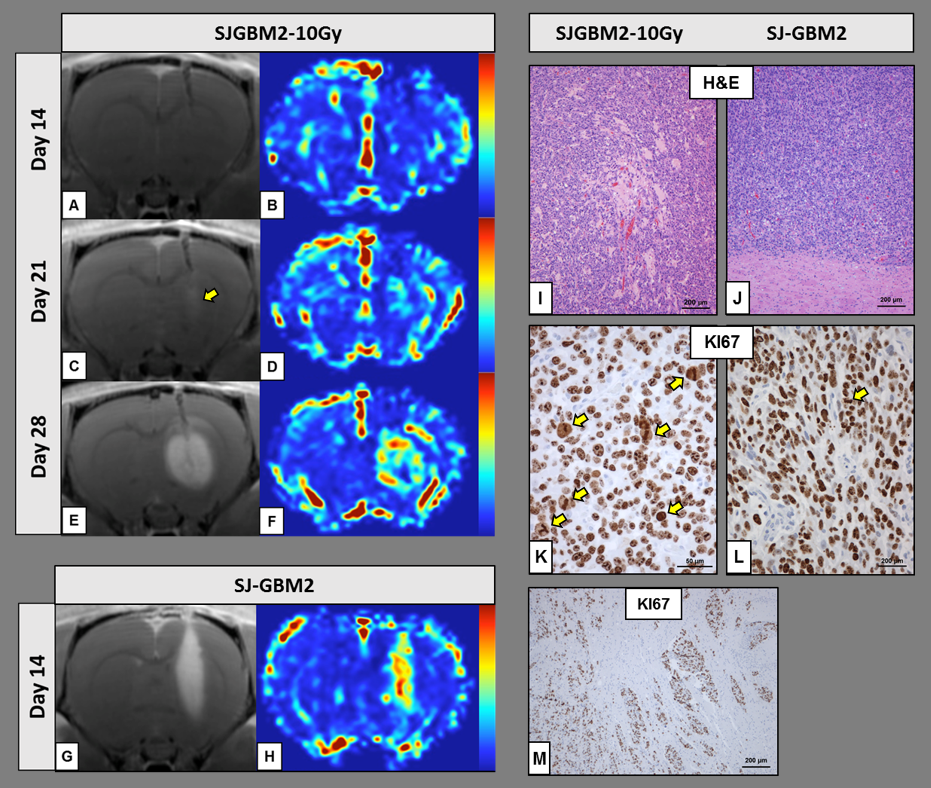
We have developed a robust and reproducible rat xenograft model of recurrent GBM by irradiating adult and pediatric GBM cell lines in vitro prior to brain inoculation. Both advanced MR imaging and histological analyses highlight the amplified aggressiveness of the resultant tumor compared to the conventional U-87MG xenograft, as evidenced by profound vascularization and increased cell proliferation. Moreover, our recurrent GBM model exhibited invasive lesions with areas of infiltrating neutrophils and necrosis, all features that are not associated with conventional U-87MG xenograft tumors. Shortened survival of animals bearing irradiated U87-10Gy or SJGBM2-10Gy tumors further reinforces the aggressive nature of the model.
Introduction
Recurrent or progressive glioblastoma (rGBM) frequently exhibits a vastly different biological behavior than de novo glioblastoma (GBM), thus making treatment for rGBM challenging, a factor that likely contributes to its poor prognosis.1 Therefore, clinically relevant preclinical models of rGBM are crucial for studying this devastating disease. Current approaches to model rGBM include in vitro drug testing,2,3 as well as in vivo irradiation,4 resection,5 or chemotherapy.6 However, the in vitro models frequently lack biological context, while the in vivo models primarily reflect treated de novo tumor, or are time-consuming and require highly specialized surgical skills. Here, we present an entirely new rat xenograft model of rGBM, which is grown from pretreated tumor cells and characterized with advanced MRI methods that distinguish tumor growth from treatment effect.
Methods
Animals: Care of the animals before and during the experimental procedures was conducted in accordance with the policies of the NIH Health Guide for the care and use of laboratory animals. All protocols were approved by the Institutional Animal Care and Use Committee at the Medical College of Wisconsin. Irradiated adult (U-87MG) and pediatric (SJ-GBM2) GBM cells were generated by exposure to five daily doses of 2Gy for a total radiation dose of 10Gy. The resultant irradiated U87-10Gy and SJGBM2-10Gy cells were tested for cell viability and allowed to reach confluence prior to stereotactic implantation into the right striatum of 7-week-old male athymic rats. Data Acquisition: In vivo advanced MR imaging was carried out over a three-week time course starting on day 14 after tumor implantation. All preclinical MR imaging was performed on a 9.4T Bruker BioSpec system fitted with a linear transmit and a 4-channel receive coil. Data collected included pre- and post-contrast T1W anatomical images, diffusion-weighted imaging (DWI), and dynamic susceptibility contrast imaging (DSC). The T1W (RARE) sequence was collected with TR=1000ms at minimum TE, flip-angle=90 degrees, 18 slices with slice thickness=0.5mm, inter-slice gap=0mm, acquisition-matrix=256x256, and FOV=3.5cm. The DWI was collected at 8 b-values (50, 100, 150, 200, 400, 800, 1000, 1500 s/mm2), with TR=4,500ms, TE=30-50ms, flip-angle=90 degrees, 9 slices with slice thickness=0.7-1mm, inter-slice gap=0-0.3mm, acquisition-matrix=128x128, and FOV=3.5cm. Following 0.2 mmol/kg gadodiamide (Omniscan™: GE Healthcare Inc., Princeton, NJ) contrast agent administration, a post-contrast T1W (RARE) anatomical scan was collected. To obtain dynamic relative cerebral blood volume (rCBV) measures, DSC gradient-echo echo-planar imaging (DSC GRE-EPI) was acquired with TR=1000 ms, TE=16/33ms, flip-angle=75-90 degrees, 9 slices with slice-thickness=0.7-1mm, inter-slice gap=0-0.3mm, acquisition-matrix=128x128, and FOV=3.5 cm. The DSC contrast injection (5 mg/kg MION; courtesy of Dr. Young Kim, Massachusetts General Hospital, Charlestown, MA) occurred exactly 60 seconds into the DSC scan at a rate of 10 ml/min using a power-injector. Image & Data Analysis: For this study, advanced MRI parameter maps, including the distributed diffusion coefficient (DDC),7 rCBV (determined from the dynamic MION injection scans), and T1 subtraction maps, were processed for enhancing tumor ROIs in OsiriX 8.5.1 (Lite) with Imaging Biometrics™ Software (Imaging Biometrics LLC, Elm Grove, WI). Fractional tumor burden (FTB) maps were constructed as previously described.8 Kaplan-Meier survival curves (Gehan-Breslow analysis) for the three U-87MG and five U87-10Gy rats were created in SigmaPlot 11.0. The level of significance was set at p=0.05. Immunohistochemical staining (H&E for anatomy and cellularity, KI67 for proliferation, and von Willebrand Factor for vasculature) was performed according to standard protocols by the CRI Histology Core at the Children’s Hospital of Wisconsin.Results
The study results are summarized in Figures 1 through 4.Discussion
We have developed an expedient, yet robust and reproducible, rat xenograft model of rGBM by irradiating GBM cell lines in vitro prior to brain inoculation. Both advanced MR imaging and histological analyses highlight the amplified aggressiveness of the resultant tumor compared to the conventional U-87MG xenograft. Our rGBM model exhibited invasive lesions with areas of infiltrating neutrophils and necrosis, all features that are not associated with conventional U-87MG tumors.9 Shortened survival of animals bearing U87-10Gy xenograft tumors further reinforces the aggressive nature of model. We were able to reproduce similar features using the pediatric SJ-GBM2 cell line. However, because those cells were obtained from a previously treated GBM, following in vitro irradiation we observed xenograft tumors exhibiting one of two phenotypes (invasive or angiogenic). This is a finding that warrants further study and characterization.Conclusion
Our novel rGBM xenograft model represents a robust and reproducible in vivo model for studying recurrent GBM biology using in vitro irradiated cell lines.Acknowledgements
Funding support was provided by NIH/NCI R01CA082500, the Daniel M. Soref Charitable Trust, and the Musella Foundation. Special thanks to the Children's Research Institute Histology Core at the Children's Hospital of Wisconsin, and to Matt Runquist of the MCW Center for Imaging Research for help with MR imaging.References
1. Fangusaro J. Pediatric high grade glioma: a review and update on tumor clinical characteristics and biology. Front Oncol. 2012;2: 105.
2. Bax DA, Little SE, Gaspar N, et al. Molecular and phenotypic characterisation of paediatric glioma cell lines as models for preclinical drug development. PLoS One. 2009;4: e5209.
3. Kang MH, Smith MA, Morton CL, Keshelava N, Houghton PJ, Reynolds CP. National Cancer Institute pediatric preclinical testing program: model description for in vitro cytotoxicity testing. Pediatr Blood Cancer. 2011;56: 239-249.
4. Perez-Torres CJ, Engelbach JA, Cates J, et al. Toward distinguishing recurrent tumor from radiation necrosis: DWI and MTC in a Gamma Knife--irradiated mouse glioma model. Int J Radiat Oncol Biol Phys. 2014;90: 446-453.
5. Hingtgen S, Figueiredo JL, Farrar C, et al. Real-time multi-modality imaging of glioblastoma tumor resection and recurrence. J Neurooncol. 2013;111: 153-161.
6. Corroyer-Dulmont A, Peres EA, Gerault AN, et al. Multimodal imaging based on MRI and PET reveals [(18)F]FLT PET as a specific and early indicator of treatment efficacy in a preclinical model of recurrent glioblastoma. Eur J Nucl Med Mol Imaging. 2016;43: 682-694.
7. Bennett KM, Schmainda KM, Bennett RT, Rowe DB, Lu H, Hyde JS. Characterization of continuously distributed cortical water diffusion rates with a stretched-exponential model. Magn Reson Med. 2003;50: 727-734.
8. Prah MA, Al-Gizawiy MM, Mueller WM, et al. Spatial discrimination of glioblastoma and treatment effect with histologically-validated perfusion and diffusion magnetic resonance imaging metrics. Journal of Neuro-Oncology. 2017.
9. Candolfi M, Curtin JF, Nichols WS, et al. Intracranial glioblastoma models in preclinical neuro-oncology: neuropathological characterization and tumor progression. J Neurooncol. 2007;85: 133-148.
Figures